Download
1 / 50
500 likes | 517 Views
Explore work-life balance challenges faced by physicians in Canada and around the world, examining gender distribution, parental leave, and career progression. Discover strategies for improving workplace climate and supporting women in medicine.

E N D
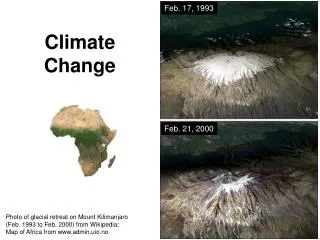
Climate Change for the Medical Workplace Lessons on physician work-life balance from around the world Janet Dollin MDCM, FCFP Kathleen Gartke, MD, FRCSC Barbara Lent MD, FCFP Cheryl Levitt MBBCh, FCFP
Outline 1. Current situation in Canada 2. International Experience 3. Planning for the future
1.Current situation in Canada • Introduction - brief overview of data on women in medicine and in med school as it relates to Canadian workforce issues • FMWC Needs Assessment 2008 & Customizing Balance call for stories- shining the light on perceptions of women in the Canadian medical workforce-what we want • Work Life Policies for Canadian Medical Faculty 2009 FMWC -shining the light on what we now have in place
1. Current situation in CanadaIntroduction Women comprise: • 70% of students in some med schools • 65% of new Fam Med grads • 58% of medical students overall • 50% of all Cdn physicians < age 35 • 30% of the Canadian medical workforce • 18% of full professors of medicine • 13% of department chairs
Current situation in CanadaWomen physicians comprise • 83% first year trainees in ob/gyn • 65% first year trainees in family medicine • 14% first year trainees in cardiac surgery • 50% of geriatricians • 48% of pediatricians • 37% of gp/family physicians • 7% of orthopedists • 5% of urologists
Current situation in CanadaGender Distribution of Physicians, by Physician Type, Canada, 1978 to 2008
Current situation in CanadaBC Physician Health Program Position Statement 2010 • Medicine and Motherhood: Can We Talk? http://www.physicianhealth.com • Workplace climate (accommodation) will impact • Maternal and fetal health. • Mother and child well-being during pregnancy and postpartum. • Female physicians career progression, career choices and practice patterns. • HHR planning
1. Current situation in CanadaNational Physician Survey 2007 • Major responsibility for children or other dependents Significant differences (p<0.05) by sex and by age for females
1. Current situation in CanadaNational Physician Survey 2007 In the last year, have you been absent from work due to maternity or paternity leave? Men 2.3% Women 7.8% ( consider absolute #s) • For men who take parental leave: 95%<16 wks • For the women who do so: 75%>16 wks • We need to plan for that
1. Current situation in CanadaNational Physician Survey 2007 Hours worked per week by type of dependents (excluding on call) -No significant difference in work hours for men and women when no dependants -Having dependent children alters work hours differently for men and women Overall 47:52 hrs F:M
Trends in the Work Hours of Physicians in the United StatesDouglas O. Staiger, PhD; David I. Auerbach, PhD; Peter I. Buerhaus, PhD, RN JAMA. 2010;303(8):747-753. % Change for US Physician hours Between 1996 and 2008 • All physicians (54.9 hrs-51 hrs) −7.2 % • Men (54.4-51.7 hrs) −5.0 % • Women (46.7-44.4 hrs) −5.1 % • Lawyers (45.9-44.9 hrs) −2.4 % • Engineers (43.6-43.0 hrs) −1.4 % • Registered nurses (36.7-37.3 hrs) +1.6 %
Generation Effect? Boomers (1945-1962) -Work hard out of loyalty -Expect long-term job -Pay dues -Self-sacrifice is virtue -Respects authority Generation X (1963-1983) -Work hard if balance allowed -Expect many job searches -Dues not relevant -Self-sacrifice may have to be endured, occasionally -Questions authority Millenials (mid 1980’s up) -Plugged in 24/7-tech and media savvy -Work hard but demand flexible schedules and a better work/life balance -Value teamwork and responsibility, desire to shape their jobs to fit their lives rather than adapt their lives to the workplace -Achievement oriented and confident but question authority, assertively seek more feedback
1.Current situation in CanadaFMWC Needs Assessment 2008 • The FMWC -a unified voice for Canadian female physicians • promote interests of female physicians • improve management of women’s health issues • The 2008 Needs Assessment was an online survey of its members designed to understand the priority issues for women in medicine and to aid in design of its new website. It offers us a glimpse at the concerns these women have about the current situation in Canada…
1.Current situation in CanadaFMWC Needs Assessment 2008 Improve workplace flexibility, job sharing, part-time work and ensure this flexibility is equitably available across all specialties Increase physician resources in Canada and stop identifying women in medicine as the cause of human health resource problems The increasing number of healthcare trainees dictate the need for more faculty – especially women advancing to leadership positions
Customizing Personal Balance within Medicine Call for stories 2008the questions: • How have you customized things to balance your job and personal life? • Tell us about your personal experience of less than full time work, job sharing, parental leave, re-entry experiences, Stop the clock, promotion policies, etc. • What policies within your institutions have supported you? What policies have not? • Was it a personal or group negotiation that got you what you needed to create balance? • What is it about your particular specialty that makes it easier or harder to achieve what you need?
Customizing Personal Balance within Medicine Call for stories 2008the answers by theme: 1.Balance: Was it planning or serendipity?: • Act to not allow our institutions to repeat bad experiences. Train for resilience. Mentor: seek and be a role model. Act to make ‘opting in’ the better choice. Flexible workplaces will keep the medical workforce balanced. 2.Thoughts on having children: • Attitudes towards raising families while having a career in medicine need updating. Workplaces need to be more family and caregiver friendly, which includes but is not limited to parental and caregiving leave, stop the clock advancement policies, re-entry support, etc
Customizing Personal Balance within Medicine Call for stories 2008the answers by theme: 3.The importance of personal health: • We all need time for self care, a supportive community of friends and work environments that can adapt to our health needs as care providers and that will support our indirect journeys. 4.Thoughts on careers: • Help our institutions to value less than full time and flexible work and to create more of these lifestyle friendly work opportunities. Act to allow women to lead in medicine and use their “Take charge” talents.
Work-Life Policies at Canadian Medical Schools(An FMWC & CMA Collaborative Project) Kathleen Gartke M.D. FRCSC Aaron Gropper B.Sc. Hon Monika MacClaren M.B.A. From the JOURNAL OF WOMEN’S HEALTH Published by Mary Ann Liebert, Inc, New Rochelle, NY
Rationale • Is there a problem? • Lots of literature – nothing Canadian • What is our situation? • How do we compare? • Modeled after an American study (Bristol et al 2008 – top 10 schools (US News & World Report 2006)) • Advocacy begins by defining the problem
Work-Life Policies at Canadian Medical Schools • Maternity Leave • Paternity Leave • Adoption Leave • Extension of Probationary Period for Birth or Adoption • Part time / Reduced Work Load Appointments • Job Sharing • Child Care
Work-Life Policies at Canadian Medical Schools • Data gathering • Web search • Email • Phone • Compilation • Legislation • Scoring • Analysis / Comparison
Legislation • Canadian • Federal • 17 weeks EI benefits (+35 wks unpaid parental) • Provincial (universities) • 15 weeks EI benefits (+35 wks unpaid parental) • American • FMLA • 1993 • 12 weeks of unpaid, job protected leave for specific family & medical reasons
Work-Life Policies at Canadian Medical Schools • Up to 45% of faculty (USA) have expressed thoughts of leaving (often related to concerns about balance) • Generation X (1963 – 1981) • Ability to control job outweighs salary & prestige • John Hopkins – policies to retain more women led to increased retention of men (66% & 57%)
Work-Life Policies at Canadian Medical Schools • Results • Canadian schools have much more generous maternity, paternity & adoption leaves • Wide variation in these (paid) • French language schools: most generous • University of Alberta : least generous
Work-Life Policies at Canadian Medical Schools • Results • Extension of probationary period: Canadian schools more uniformly generous than US • All offer at least one year extension • Some allow unlimited repeats, others not • No Canadian school has eliminated the pre-tenure period (gone to merit based promotion)
Work-Life Policies at Canadian Medical Schools • Results • Part time or work reduction programs: available at most Universities • Some offer only to tenured faculty • American schools : slightly better part time or work reduction policies • Job sharing: much more common in American schools
Work-Life Policies at Canadian Medical Schools • Results • Childcare: Most have on campus childcare and often offer referrals +/- financial • Northern Ont School of Medicine: no childcare • Canadian Schools: generally better than American
School University of Ottawa Total Score (out of apossible 21) 12 Average Scores (across all policies) 1.71 Université de Sherbrooke 12 1.71 University of Western Ontario 16 2.29 Université de Montreal 12 1.71 University of Manitoba 15 2.14 University of Toronto 11 1.57 University of Saskatchewan 14 2 University of Alberta 11 1.57 University of British Columbia 14 2 University of Calgary 10 1.42 Northern Ontario School of Medicine 7 1 Dalhousie University 14 2 Université de Laval 13 1.86 Queen's University 13 1.86 Memorial University of Newfoundland 13 1.86 McMaster University 13 1.86 McGill University 13 1.86
American Schools Total Scoreof all policies (out of possible 21) John Hopkins 15 University of California, San Fransisco 15 Harvard University 14 Duke University 13 Yale University 13 Stanford University 9 University of Washington 9 Baylor College of Medicine 9 Washington University in St Louis University of Pennsylvania 7 6
Work-Life Policies at Canadian Medical Schools • Standouts • U of Western Ontario: • Highest score • Has a unique “work-life balance” section on website • Frequently addresses issues of balance • Northern Ontario School of Medicine • Lowest score • Least generous policies in several areas
Work-Life Policies at Canadian Medical Schools • Conclusions • Canadian medical schools are committed to helping staff achieve work-life balance • Policies have improved (quality & accessibility) • Further improvement possible & desirable • Culture change • Attract & retain the best
“Although we may define ourselves first by what we do, it is those personal relationships outside of work that make us whole” John Curtis (Academe, Nov/Dec 2004)
2.International Experience Making Part Time Work-2008 UK MWF and EU working time alliance Women Doctors:Making a Difference-2009 UK MWF report Achieving gender equity from within:Wonca WPWFM HER statement & “Gender Equity Standards for Scientific Meetings”
2.International Experience UKMWFMaking Part Time Work-2008 1.Recommendations on attitudes to part time working • Systemic attitude changes through role models, mentors and case studies as well as formal consultation with those doctors trying new work plans 2.Recommendations on part time career grade posts • Royal College guidance sought and leadership from Medical Directors needed to create flexible teaching positions 3.Recommendations on career development for pt doctors • Formal re-entry after career break, formal feedback with those who are in part time posts 4.Recommendations on part time training posts • Medical directors should promote innovative job design as well as informing and supporting those part time workers using them • Colleges and employers must collaborate to ensure coverage
2.International Experience UKMWFMaking Part Time Work-2008 • European Working Time Directive • In 2008 the maximum # working hrs per week recommended by the EWTD was 56 • In 2009 it was reduced to 48 (35 in France!) • Opens debate about the negative impacts of long hours on performance vs the needs for “putting in the hours” needed to learn • Setting a ceiling on maximum work time is only part of the story
2.International Experience-UKMWFWomen Doctors:Making a Difference-2009 • Previous reports focused on desired outcomes rather than the necessary levers of change to achieve them • Narrow and targeted recommendations:
2.International Experience UKMWFWomen Doctors:Making a Difference-2009 • Improve existing structures so that there is better advancement to certain critical career turning points as well as different ways of working • Ensuring that new processes (such as revalidation) have the flexibility and capacity to accommodate doctors who may not be conforming to the usual work patterns • Providing additional support for the practical realities of caring for a child or dependent relative
2.International Experience UKMWFWomen Doctors:Making a Difference-2009 • Improve access to mentoring and career advice • Encourage women in leadership • Improve access to part time working and flexible training • Ensure that the arrangements for revalidation are clear and explicit • Women should be encouraged to apply for Clinical Excellence Awards • Ensure medical workforce planning apparatus takes account of increasing number of women in the medical profession • Improve access to childcare • Improve support for carers • Strenuous efforts should be made to ensure that these recommendations are enacted through the identification of champions
Sir Liam Donaldson Chief Medical Officer,England “The issues raised are not new, nor perhaps are they unexpected. But to tackle them is going to require a step change in how the medical workforce as a whole behaves. It will require an acceptance of alternative and differing patterns of working and training for all medical staff, not just women…”
2.International ExperienceAchieving gender equity from within:Successes and challenges in promoting the perspective of the Wonca Working Party on Women and Family MedicineBarbara Lent Cheryl Levitt
Goals To describe how a small group of very committed women family physicians from around the world came together worked “from within” to ensure their international, organized body better reflected their experiences To delineate key successes To describe the factors that helped to make their efforts successful To discuss lessons learned from this work
Background Individually and in informal small groups, women family doctors recognize that organized medicine (particularly, family medicine): Lacked adequate representation of women in leadership positions Did not provide them with adequate education/training to address their women patients’ concerns Did not accommodate their family/household responsibilities well Convened scientific meetings with few women physicians as experts and few sessions addressing clinical issues from a gender issues perspective
Key Accomplishments The HER statement (Hamilton Equity Recommendations) addresses governance issues within Wonca 10 Steps to Gender Equity in Health describes fundamental issues, taking into account particular social circumstances facing women Gender Equity Statement for Scientific Meetings articulates key principles for organizing committees to consider Monograph/Literature Review a comprehensive review of articles in international scientific literature addressing particular issues facing women physicians/medical trainees in educational, clinical and organizational settings
Publications Peer-reviewed professional journals (scientific articles, news items, commentary) relevant professional newsletters (Wonca News; newsletter of Federation of Medical Women of Canada) Website: womenandfamilymedicine.com Self-publication: large brochure distributed to colleagues to highlight group’s activities/successes
Drivers of Success (1) 1. Working within existing Wonca organizational structure (from informal lunch-time meetings to Special Interest Group to Working Party) 2. Fostering relationships with like-minded physicians from around the world 3. Building capacity and leadership development through pre-conferences and special workshops at regular meetings, with particular attention to needs of younger physicians
Drivers of Success (cont’d) 4. Consistently applying an evidenced-based approach 5. Using technology to enhance communication (eg listserve, website, teleconferences by SKYPE) 6. Developing creative responses to financial inequities (eg bursaries specific to WWPWFM; travel equalization to enable participation by members from developing countries)
Lessons Learned Use a “bottom-up” approach so that new initiatives reflect physicians’ experiences with patients, in organizations, with colleagues Pursue a slow, consistent, persistent approach! Collaborate with like-minded colleagues, recognizing that “the sum is greater than parts” Build on the energy and commitment that comes from long-term relationships with like-minded colleagues Bring relevant info/perspective from non-medical organizations Follow/copy the path of other successful groups Frame discussion of gender issues in a way that is relevant to the parent organization
3. Planning for the Future Conclusions Where would we like to go?