Download
1 / 15
160 likes | 316 Views
Reproductive and endocrine disease. Shujun Gao. Individual. Each in normal position Each keeps normal activity Each has normal reaction. System. Normal——interaction in balance Dysfunction——lost of balance. Center stratum cutaneum. ?. Reproductive endocrine axis.

E N D
Reproductive and endocrine disease Shujun Gao
Individual • Each in normal position • Each keeps normal activity • Each has normal reaction
System • Normal——interaction in balance • Dysfunction——lost of balance
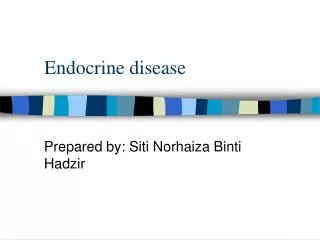
Center stratum cutaneum ? Reproductive endocrine axis Inferior colliculus GnRH Pituitary gland Gonadotropin FSH LH progestogen estrogen
amenorrhea • xxx, 16-year-old with secondary sexual characters ,but absence of menstruation • Question :What is the diagnosis and how to treat?
Correlated knowledge • The initiate and maintain of the normal menstruation • Normal growth sequence of puberty • Conditions of ovarian growth • Physiologic function of ovarian • Methods of examination of ovarian function
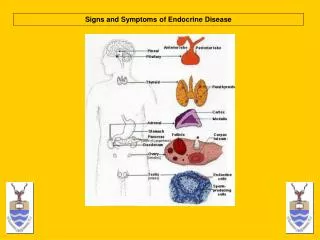
Causation and pathophysiology • Hypothalamic amenorrhea • Pituitary amenorrhea • Ovarian amenorrhea • Uterine amenorrhea • Congenital dysplasia of low genital tract • Dysfunction of other endocrine glands
Definition • It is a common symptom ,not a disease • Primary amenorrhea: secondary sexual characters not appears after 14-years or no menarche after 16-years although secondary sexual characters appeared. • Secondary amenorrhea:cessation of the periods for 6months after menstruation has been established
Classification (one) • Primary amenorrhea——most due to congenital diseases or functional disorder and deformed genital tract,about 5%。 • Secondary amenorrhea——most due to secondary dysfunction or tumor,about 95%。
Classification (two) • Physiologic amenorrhea • Pathological amenorrhea
Classification (three) According to the anatomic site • Congenital dysplasia of low genital tract • Uterine amenorrhea • Ovarian amenorrhea • Pituitary amenorrhea • Central nerve-hypothalamic amenorrhea
Classification (four) According to the level of sex hormone • Hypergonadotropic hypogonadism: FSH≥30IU/L,lesion presence in ovarian • hypogonadotropic hypogonadism: FSH and LH both<5IU/L,lesion presence in center
Dysfunctional uterine bleeding • Patient ——Troubled by dysfunctional uterine bleeding sees a doctor to resolve bleeding and to get normal menstruation • Doctor —— you, should know how to satisfy the patient • To solve the problem, diagnosis, differential diagnosis and treatment should be mastered
Patient: 17-year-old , 46kg • Chief complaint:menstrual disorder for 2 months,vaginal bleeding for 18 days • Menstruation: 11year 5-7/20-30days。Pmp 2007.07.03 ,Lmp 2007 08.24。 • History of present illness: She had a heavy vaginal bleeding from September 5th, 2007 ,accompany with dizziness, vertigo and fatigue,and was hospitalized emergency • Medical examination: T36.7、P88cpm、R21cpm、BP90/50mmg. depressed with an anemia face • Gynecology examination: corpus:middle position with normal size adnexa:no masses • ultrasound: UT46× 45×40mm, EN10mm ROV31×28×23mm, LOV33×17×16mm. Cul-de-sac hydrops:18mm.
discussion • diagnosis:puberty dysfunctional uterine bleeding secondary anemia • Procedure of diagnosis: history of illness medical examination gynecological examination auxiliary examination:urine HCG、 ultrasound、 sex hormone、blood routine. • Therapeutics:sex hormone diagnostic curettage antibiotics treatment of anemia