Download
1 / 26
361 likes | 1.4k Views
Oxygen Therapy. Dr Surinder Singh IGMC Shimla. Basic Concepts:. Oxygen Cascade : Inspired = 150 mmHg at Sea Level SML120 ↓ Alveolar PO 2 = 103 ↓ Arterial=100 ↓ Capillary= 51 ↓ Mitochondrial= 1-10 (FiO 2 expressed as 0.21-1.0 or 21- 100%). Oxygen Availability: Normal.

E N D
Oxygen Therapy Dr Surinder Singh IGMC Shimla
Basic Concepts: Oxygen Cascade: Inspired = 150 mmHg at Sea Level SML120 ↓ Alveolar PO2= 103 ↓ Arterial=100 ↓ Capillary= 51 ↓ Mitochondrial= 1-10 (FiO2 expressed as 0.21-1.0 or 21- 100%)
Oxygen Availability: Normal Oxygen Flux or O2 availability/min: = (Hb content+ Plasma content) x Q = (1.39x Hb x SaO2 + 0.003 x PaO2 ) x Q ml 100 100 = (1.39 X 14.5 X 97.5+.003 X 100) X 5000 100 100 = 985+ 15 = 1000ml Coefficient of Oxygen utilisation: O2 consumed/ O2available = 250 =25% Safety margin= 75% 1000
Oxygen Availability: Disease state • Low CO eg. 50%+ Normal Hb = 500 ml Safety=50% • Low CO eg 50%+ Low Hb 7gm= 250 ml Safety=?? • Hemorrhagic Shock= ↓CO+↓Hb=↓↓↓↓ O2 • MS+Anemia= ↓CO+↓Hb=↓↓↓↓ O2 Critical Flux= 500ml Last 250ml can’t be extracted The narrow safety margin is further reduced if oxygen demand increases in such patients
Perioperative State: ↑ Oxygen demand due to shivering, fever, sepsis, hypercatabolic state. Patients may be unable to increase cardiac output or VE or both A vicious cycle of hypoxemia may start .
Factors ↓ O2 Availability: • Low arterial O2 content: • ↓ FiO2, ↓PaO2 • ↓ Diffusion eg ARDS, CPE • ↓ pH or acidosis • Low Hemoglobin: • ↓ Hb • ↑ COHb • MetHb • Low cardiac output states
Factors ↑ O2 Requirement: • Pregnancy: ↑ 7-8 ml/kg/min Normal=4-5 ml/kg/min • Sepsis , Hypercatabolic state • Shivering= ↑ 500% of the Normal requirements • Fever: 7% increase /oC rise of body temperature • ↑ Work of breathing • ↑ Myocardial work: Tachycardia
How to ↓O2 Consumption: • Minimize exertion • Digitalize, treat cardiac failure • Prevent & Treat fever • Under extreme circumstances: • Paralysis and IPPV • Induce hypothermia • ECMO • CPB
How to ↑ O2 availability: • Raise Arterial PaO2 &SaO2 • Oxygen Therapy • Treat Bronchospasm/ respiratory lesions • Ventilation, PEEP, CPAP • Raise Hemoglobin: • Hb: BT, Pack cell transfusion • Raise Cardiac Output: • Correct Acidosis • Correct Hypovolemia • Inotropic Support • Treat Cardiac Lesions/ Shunts
Efficacy of oxygen therapy ∆O2 /100 ml Art. Blood/percent ↑FiO2 • Diffusion Hypoxia & High Altitude3 ml • Respiratory depression3 ml • ARDS/CPE • Anemia 0.03 ml • Shock, Valve defects 0.03 ml • MetHb 0.03 ml • Cytotoxic Hypoxia 0.03 ml
General considerations PIFR: Low: Respiratory depression V High: Tachypnea, ARDS Expiratory pause Longer: Resp depression Shorter: Tachypnea ARDS
General considerations • Use mask in distress :Mouth breathing • Humidification not useful < 10LPM • Use upright posture to the extent permissible • Appropriate FiO2 to achieve Target SPO2 • Confirm oxygen delivery to the patient • Prescribe& document oxygen therapy • Monitor SpO2 ABG, Vitals, Narcosis • Diagnose and treat the underlying cause MOST INDICATIONS FALL IN EVIDENCE LEVEL-D OR C
Devices for oxygen :History BLB Mask 1938 Boothby Lovelace Bulbulian Nasal mask with reservoir
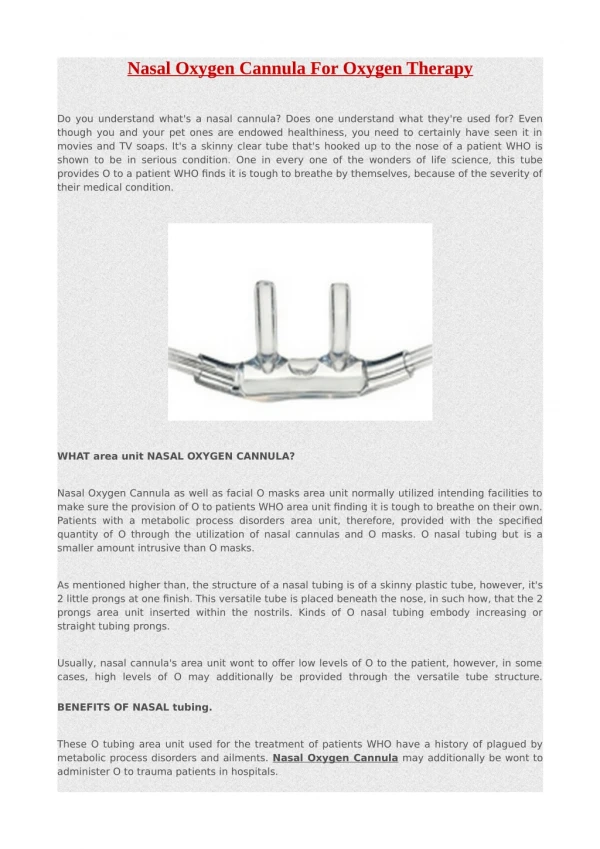
Devices Nasal Catheters:: No/ low capacity Variable performance • 2-4 LPM (BTS 2-6) • Upto 35% FiO2 Advantages: • Economical, Gas economy • No VD/ rebreathing • Eating, drinking, speaking possible • Useful for low FiO2 • Can be used in Tracheal/ Tracheostomy tube Disadvantages: • Irritation, No humidification • Encrestations, Ulceration
Nasal Prongs/ oxyarm: No/ Low capacity Variable performance Nasal Prongs: • Better tolerance • Performance same as nasal catheters • Reservoir 20-30ml • ETCO2 sampling • Oxyarm: • Cloud of 28-35% FiO2 in front of nose& mouth
Simple Mask: Low capacity Variable performance Simple Face Mask: • No limit of O2 flow • Usually 4-6 LPM • FiO2 ≈ oxygen flow • Usually 2- 4%/ LPM-1 Advantages: • Simple, No Flow limit/ FiO2 limit Disadvantages: • ? FiO2, • Cross Infection • No Humidification
Ventury masks: Fixed performance High flow Medium Conc. Mask: • Comes with one adapter set at 35% • Required 5 LPM • Set of adapters Multi Vent: One or two adjustable adapters Anaesthesia Breathing Circuits: Low flow Fixed performance
Devices:High capacity Reservoir mask • 60 – 95% FiO2 • FiO2 dependant on FGF • Inversely related toVË • Rebreathing directly related toVË and inversely related to FGF • Valve between the reservoir & mask prevents rebreathing • Requires continued flow and observation
Hood, tent and Incubator • Large capacity for oxygen and CO2 • Unpspecified FiO2
Oxygen Toxicity: Described by Sir joseph Priestley Generation of Superoxide radicals O - Absorption atelectasis ↓ Surfactant production Drying of mucosal epithelium and secretions ROPM, Fibrocystic dysplasia, ARDS ↑ PCO 2 in COPD patients: Narcosis • FiO 2 100%= 4 hrs FiO 2 80%= 8 hrs • FiO 2 70%= 12 hrs FiO 2 60%= 24 hrs • FiO 2 ≤ 50%= Indefinite
Choose wisely - live well THANKS FOR YOUR PATIENT LISTENING