Download
1 / 16
160 likes | 267 Views
600 East Superior Street, Suite 404 I Duluth, MN 55802 I Ph. 800.997.6685 or 218.727.9390 I www.ruralcenter.org . Tying it All Together Using EMRs to Support Quality Improvement. Joe Wivoda CIO December 6, 2013. About The Center.

E N D
600 East Superior Street, Suite 404 I Duluth, MN 55802 I Ph. 800.997.6685 or 218.727.9390 I www.ruralcenter.org Tying it All Together Using EMRs to Support Quality Improvement Joe Wivoda CIO December 6, 2013
About The Center The National Rural Health Resource Center is a nonprofit organization dedicated to sustaining and improving health care in rural communities. As the nation’s leading technical assistance and knowledge center in rural health, The Center focuses on five core areas: • Performance Improvement • Health Information Technology • Recruitment & Retention • Community Health Assessments • Networking
About Me I have worked in IT for 20 years, HIT for 15 years in various roles, including consultant, CIO, developer, and project manager • HIT Consultant for MN/ND Regional Extension Center • Rural HIT Network Technical Assistance • TASC HIT Consultant • Working with multiple HIEs • Worked with an HIT Vendor to achieve certification and improve service delivery
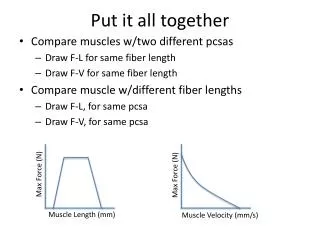
2014 Quality Measures and EHRs • “The Devil’s in the Details” • Quality measures are detailed on the National Quality Forum (NQF) website • http://www.qualityforum.org • Numerator, denominator, exclusions are all defined there • Your EHR will not automatically do this for you!
The details… Where are these documented? Is that where the vendor EXPECTS them? • Numerator: • Patients who received VTE prophylaxis or have documentation why noVTE prophylaxis was given:? the day of or the day after hospital admission? the day of or the day after surgery end date for surgeries that start the day of or the day afterhospital admission • Denominator: • All patientsInclusions: Not applicable • Exclusion: • Patients:? Patients less than 18 years of age? Patients who have a length of stay (LOS) < two days and > 120 days? Patients with Comfort Measures Only documented? Patients enrolled in clinical trials? Patients who are direct admits to intensive care unit (ICU), or transferred to ICU theday of or the day after hospital admission with ICU LOS = one day? Patients with ICD-9-CM Principal Diagnosis Code of Mental Disorders or Stroke asdefined in Appendix A, Table 7.01, 8.1 or 8.2? Patients with ICD-9-CM Principal or Other Diagnosis Codes of Obstetrics or VTE asdefined in Appendix A, Table 7.02, 7.03 or 7.04? Patients with ICD-9-CM Principal Procedure Code of Surgical Care ImprovementProject (SCIP) VTE selected surgeries as defined in Appendix A, Tables 5.17, 5.19,5.20, 5.21, 5.22, 5.23, 5.24 Source: NQF 0371 from National Quality Forum – http://www.qualityforum.org
Chaudhry B, et al. (2006). "Systematic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care." Annals of Internal Medicine.
Quality of Diabetes Care: Patients Treated by Physicians using EHR vs. Paper Medical Records Standard Protocols Reminders % of Patients Receiving Care A significantly higher proportion of patients being treated by physicians with EHRs received care that aligns with accepted treatment standards * Source: Cebul, R. D., M.D.; et al. (2011). Electronic Health Records and Quality of Diabetes Care. New England Journal of Medicine, 365:825-833. Retrieved from http://www.nejm.org/doi/full/10.1056/NEJMsa1102519#t=article * Even after adjusting for patient demographic characteristics and insurance type, differences remain significant; p<0.001
Example: Aspirin prescribed at discharge for AMI (NQF 0142) • Numerator: AMI patients who are prescribed aspirin at hospital discharge • Denominator: AMI patients (ICD-9-CM codes 410.00, 410.01, etc) • Exclusions: MANY!
Exclusions for NQF 0142 •<18 years of age•Patients who have a length of stay greater than 120 days•Patients enrolled in clinical trials•Discharged to another hospital•Expired •Left against medical advice•Discharged to home for hospice care•Discharged to a health care facility for hospice care•Patients with comfort measures only documented •Patients with a documented reason for no aspirin at discharge
Consider One Exclusion • Exclusion: Patients with a documented reason for no aspirin at discharge • Where will that be recorded? • Is that where the EHR is looking when it does the report? • Who might enter that data? Nursing? Physician?
Possible workflow for AMI Patient Where is this documented? Is it discrete or in a note? Is this discrete? Is this a sufficient indicator that aspirin is not advisable? Will the EHR look there when doing the report??
Improved Workflow for AMI Patient “Reason code” populates correct area of database so CQM will calculate correctly
“Doesn’t 2014 EHR Certification fix this?” • “EHR technology must be able to electronically calculate each and every clinical quality measure for which it is presented for certification” • From “Testing tool for Electronic Health Record Software Certification, 2014 Edition, Criteria 170.314(c)” • Nothing specifies that the data elements need to be easy and straightforward to enter or retrieve • Nothing specifies the process for getting the data into the EHR to allow the CQM to calculate correctly.
Next Steps • Process improvement and understanding your EHR are critical • Do you have a PI methodology in place? (Lean/PDCA/Tracer) • Is your quality leader involved? • Vendor involvement and test/training system • Talk to your vendor • Utilize your test system (is it up to date?)
Useful Websites National Quality Forum: http://www.qualityforum.org Hospital Compare Data Specifications (Search for Specifications Manual) http://www.qualitynet.org ONC-CHPL: http://onc-chpl.force.com ONC’s Health IT Site http://Healthit.gov National Rural Health Resource Center http://www.ruralcenter.org
Joe Wivoda • CIO & HIT Consultant • National Rural Health Resource Center • 600 East Superior Street, Suite 404 • Duluth, MN 55802 • (218) 262-9100 • jwivoda@ruralcenter.org