Download
1 / 12
120 likes | 160 Views
Learn about lateral and high ankle sprains, grading, symptoms, and treatment options for Dwight Freeney's recent injury. Understand the role of hyperbaric oxygen therapy and electrical stimulation in ankle rehabilitation. ###

E N D
Nathan McNeil, MD CAQ in Sports Medicine Ankle sprains
Anatomy AJR Am J Roentgenol 138:683, 1982
Dwight Freeney • Injured right ankle in AFC championship game • He’s been in a walking boot all week • Reports are that he has a torn ligament on the lateral (outside) part of his ankle • He’s been using Hyperbaric oxygen treatments as well as an “ARP device”
Lateral Ankle Sprains • The Anterior talofibular ligament (ATFL) is the most common ligament injured. • The Calcaneofibular ligament (CFL) may also be injured • The injury is graded from I-III based on laxity (instability), swelling and pain with weight-bearing. • Caused when an athlete inverts (rolls inward) his ankle
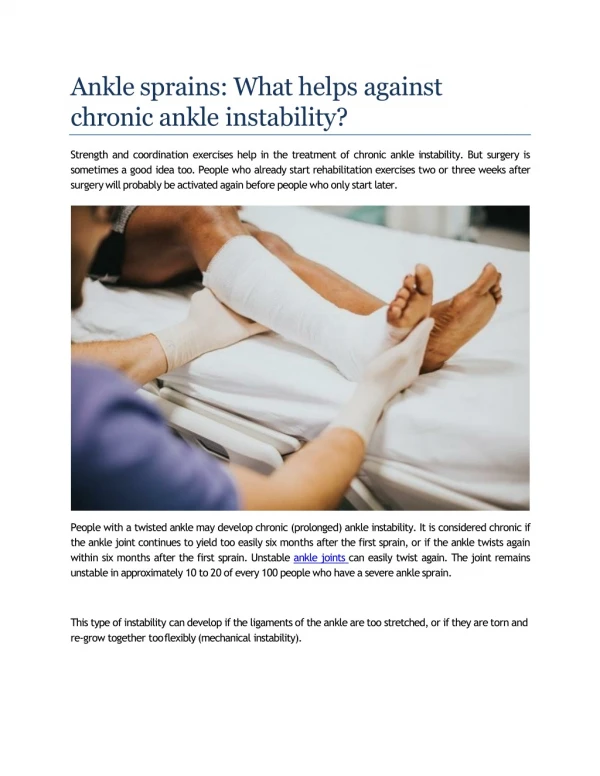
High Ankle Sprains • Less common injury caused by eversion (roll outward) and external rotation of the ankle • The force gets transferred through the syndesmosis (intraosseus membrane) and the tibiofibular ligaments that hold the tibia and fibula together.
High Ankle Sprains • This injury is much more serious because it may result in diastasis (spreading) of the ankle joint with weight-bearing. • Depending on the severity, it may be treated with syndesmotic screws (figure to left) or casting and crutches www.wheelessonline.com
Discussion • Dwight Freeney appears to have the less serious lateral ankle sprain • Compare to Terrell Owens who had a severe variation of the “high ankle” sprain associated with a fibular fracture called a Masionneuve injury. • According to ESPN reports Dwight Freeney has a grade III (complete ligament tear) injury. • He is currently listed as questionable and his ability to play is dependent on his ability to regain stability, strength and pain-free motion
Discussion--Rehab • According to reports from ESPN, Dwight Freeney has been using hyperbaric oxygen treatments as well as an ARP device. • Hyperbaric oxygen therapy uses increased oxygen concentration and pressure in a chamber • It’s typical application is for treatment of a diving side effect called decompression sickness or “the bends” • It’s also commonly used to promote wound healing, particularly with anaerobic infections
Discussion--Rehab • To date, there is no convincing evidence that hyperbaric oxygen therapy helps ankle sprains • A randomized double-blind study of 32 subjects with acute ankle sprains to compare treatment with hyperbaric oxygen at 2 atmospheres absolute pressure (N = 16) (treatment group) with treatment with air at 1.1 atmosphere absolute pressure (N = 16) (control group) in a hyperbaric chamber. Each group received three treatments at their respective pressures : one for 90 minutes and two for 60 minutes each. Mean age, severity grade, and time to treatment (treatment group, 34.3 ± 6.3 hours; control group, 32.6 ± 4.6 hours) were similar in both groups. Joint function measured by a functional index improved from 0.40 ± 0.2 to 6.3 ± 0.4 with hyperbaric oxygen and from 0.8 ± 0.3 to 5.3 ± 0.6 with air. The change from initial to final evaluation was significantly greater in the treatment group. Foot and ankle volume by water displacement decreased from 1451 ± 57 ml to 1425 ± 63 ml with hyperbaric oxygen and from 1403 ± 50 ml to 1371 ± 45 ml with air (no difference was noted between hyperbaric oxygen treatment and air treatment using a two-way analysis of variance). Subjective pain index fell from 3.3 ± 0.5 to 0.8 ± 0.3 with hyperbaric oxygen and from 2.6 ± 0.3 to 0.3 ± 0.2 with air. No differences were noted in passive or active range of motion when comparing hyperbaric oxygen treatment with air treatment. Time to recovery was the same in both groups (treatment, 16.0 ± 6.3 days; control, 15.4 ± 2.8 days). Regression analysis to determine the influence of time to treatment, initial severity of injury, hyperbaric oxygen, and age showed no effect of hyperbaric oxygen treatment on time to recovery. Am J Sports Med September 1997 vol. 25 no. 5 pp 619-625
Discussion--Rehab • The ARP device that Freeney is using is a form of electrical stimulation. • In general, electrical stimulation is thought to relieve pain and inflammation, strengthen muscle, and reduce abnormal muscle tone. • However, there is no good evidence that it significantly contributes to faster rehabilitation PHYS THER Vol. 87, No. 1, January 2007, pp. 53-65
Ankle Rehab Evidence • A review of effective treatments published in 2008 • They asked which intervention(s) best augment early mobilization and external support after an acute ankle sprain? • What is the most appropriate method of preventing re-injury? • Design: A systematic review of randomized controlled trials published from 1993 to April 2005. Participants: People with an acute ankle sprain. Intervention: Any pharmacological, physiotherapeutic, complementary or electrotherapeutic intervention added to controlled mobilization with external support. Immobilization, surgical intervention, and use of external ankle supports in isolation were excluded. Outcomes: Pain, function, swelling, re-injury, and global improvement; assessed at short, intermediate, and long-term follow-up. Results: 23 trials were included with a mean PEDro score of 6/10. There was strong evidence that non-steroidal anti-inflammatory drugs can reduce pain and improve short-term ankle function. There was moderate evidence that neuromuscular training decreases functional instability and minimizes re-injury; and that comfrey root ointment decreases pain and improves function. There was also moderate evidence that manual therapy techniques improve ankle dorsiflexion. There was no evidence to support the use of electrophysical agents or hyperbaric oxygen therapy. Very few long-term follow-ups were undertaken, and few studies focused on preventing long-term morbidity. Conclusions: Non-steroidal anti-inflammatory drugs, comfrey root ointment, and manual therapy can significantly improve short-term symptoms after ankle sprain, and neuromuscular training may prevent re-injury. More high quality studies are needed to develop evidence-based guidelines on ankle rehabilitation beyond the acute phases of injury management Australian Journal of Physiotherapy. 54(1):7-20, 2008
Conclusion • Dwight Freeney is a right DE, thus he will need to push off his right ankle to attack Drew Brees • At present time, there is no evidence that ARP or hyperbaric oxygen therapy will significantly increase his chance of faster recovery • By playing, it’s unlikely he will risk significant further injury; however, his explosiveness and mobility will be decreased