Download
1 / 32
350 likes | 625 Views
Use of ankle support orthoses to prevent lateral ankle sprains in military personnel. Ted Croy Al Strickler Jose Mattos Anna Sedney. Ankle injuries in military personnel . Military service: intensive physical training Initial Entry Training Cadet training Airborne Training

E N D
Use of ankle support orthoses to prevent lateral ankle sprains in military personnel Ted Croy Al Strickler Jose Mattos Anna Sedney
Ankle injuries in military personnel • Military service: intensive physical training • Initial Entry Training • Cadet training • Airborne Training • Physical demands • Running, sports, obstacles, carrying equipment, landing from parachuting jumps • High rates of ankle injuries • Ankle injuries reduce performance, individual readiness, unit readiness • Stretching/tearing of ligaments • Compromised joint stability • Military health concern
Military Ankle Injury Background • US Military Academy (West Point): longitudinal study of 104 ankle sprains. Gerber et al. 1998 • 6wks 95% returned to full function and 100% by 6mos • 40% had persistent symptoms • 8 year retrospective cohort study on lateral ankle sprains • active duty US military Cameron et al. J Athl Train, 2010 • Ankle sprain incidence rate 34.95 per 1000 person years. • Defense Medical Surveillance System • IR is 5 times higher than studies reported in civilian population • Females are 21% more likely to sustain ankle sprain than males • $16 million spent in treatment of ankle sprain related injuries alone in military servicemembers. Gregg S. 2008
Ankle Injury Background • US Army Center for Health Promotion and Preventive Medicine • Recommended use of prophylactic ankle braces for unit level sports • “Wear semirigid ankle braces for high-risk activities (recommended).” Bullock et al. 2009 • Mandatory for certain military parachuting missions • Lateral ankle sprains in sports are the main cause of post-traumatic ankle osteoarthritis and are associated with ligament instability. Valderrabano et al. AJSM, 2005
Prophylactic Ankle Bracing • Ankle brace use reduced lateral ankle sprains in military parachutist trainees. Amoroso, J Trauma, 1998 • Non-brace wearers RR 6.9 versus brace wearers • Soldiers are authorized to wear lace-up ankle braces while in military physical training uniform. • SECDEF is authorized to institute injury prevention measures as a means to improve military health readiness
Paratrooper use of lateral ankle braces prior to airborne mission. Amoroso, Parachute Injury Brace Injury Surveillance, 2005
ASO ankle support • Nylon, laceup ankle supportive orthosis that is worn over the sock and inside the athletic shoe/cleat • It is unknown if the use of this brace reduces the incidence rate of ankle sprains in soldiers engaged in “high-risk” activities.
Purpose • Conduct RCT • Randomized to company (n=100 per company) • Issue braces • Measure new cases of lateral ankle sprain • Compare
Intervention • Mandatory brace use for all “high-risk” activity during Initial Entry Training • Running • Competitive team sports: soccer, basketball, football • Obstacle course • Rifle range • Monitor reports of ankle injuries at Troop Aid Stations
Objective • Our Objective is to test the hypothesis, using RCT, that an ankle orthotic will significantly reduce the risk of first time ankle injury among military trainees when engaged in high risk activities. • Hypothesis testing: • Null (H0): Cexposed=Cunexposed • Alternative (H1): Cexposed≠Cunexposed
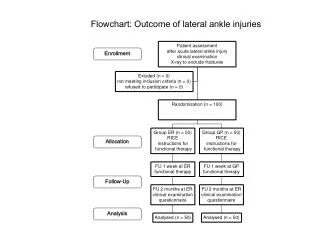
Methods Overview • 1. Randomize • 2. Issue braces and train in use • 3. Measurements over 1 year • 4. Comparisons • 5. Analyze
Methods Overview Randomize Training Companies FY2012 Brace No Brace Entry Physical Begin Initial Entry training Receive Brace Issue and Training No Brace Issue (+) Lateral Ankle Sprain (-) Lateral Ankle Sprain (+) Lateral Ankle Sprain (-) Lateral Ankle Sprain
Randomization • Company (n=100 per company) • A new company enters each week. • Each company trains for 8 weeks. • Prospective random assignment of each company to brace (treatment) or no brace (control). • Partial Blinding
Brace Use • Mandatory training • Mandatory brace use for all “high-risk” activity during Initial Entry Training • Running • Competitive team sports: soccer, basketball, football • Obstacle course • Rifle range
Measurements • Monitor total time that recruits are participating in high risk activities (person-days [PD’s]) • By 8 week company training time. • Monitor reports of ankle injuries at Troop Aid Stations • Record values for total PD’s at risk and first time ankle injuries in each group • Prospectively identify covariates to be accounted for: • Stratify and use multivariate analysis • Age • Sex • Race • Time of year
Comparisons • Combined data • Crude Incidence rates • Absolute Rate differences with CI’s (0) • Incidence rate ratios with CI’s (1)
Analysis • Attributable risk (AR): the absolute reduction in the risk of first ankle injury in military recruits wearing a brace that can be attributed to wearing a brace. • AR=Cunexp-Cexp • Population attributable risk (PAR): the absolute reduction in the risk of ankle injury in the military recruits that can be attributed to the wearing a brace. • PAR=Cpop-Cexp • Attributable risk percent (AR%):the percentage reduction in the risk of the first ankle injury in military recruits wearing a brace attributed to wearing a brace. • AR%=(Cunexp-Cexp)/Cunexp*100 • Population attributable risk percent (PAR%): the percentage reduction in the risk of first ankle injury in the military recruits attributed to wearing an brace. • PAR%=(Cpop-Cexp)/Cpop*100
Analysis • Final hypothesis testing: • Determine p-value and compare to our set significance level of p=0.05
Analysis: Other Concerns • Other side effects • Assess at medical visits and when necessary • Cost benefit analysis • Subjective feedback analysis
Traditional Limitations to RCTs • loss to follow-up • non-compliance • non-blinding • ethical • feasibility • cost
blinding impossible • possible reporting bias
Bias • confounding • randomization • base-wide enrollment • selection bias • base-wide enrollment • subjects have baseline physical fitness • information bias • most likely possible source of bias
Limitations • sources of bias • randomization by company, not individual • global differences in training regimen
large number of healthy prescreened subjects being randomized should overcome many possible sources of bias
will have to follow possible increase in other injuries - side effects of or caused by braces • identify first vs recurrent ankle injuries
homogenous test population • results may apply to military but may not generalize outside
Personnel • Recruit Battalion Commanders • Troop Aid Station physician assistants, medics, providers • Drill Instructors: train on fit/use of ASOs. • Trainees: train on fit/use
Resources and Time-Frame • We approximate new cohorts of 100 soldiers every week • Our budget will allow for 5,000 braces • Approximately $20 per brace = $100,000 • Study will last approximately one year, or until we use all 5,000 braces
Human Subject Issues • Military personnel are a special population • Injury prevention interventions are appropriate and authorized • Including helmets, uniforms, AND medical experiments • Still requires Army Medical Department IRB approval • In addition to commanding general approval and medical post at site • The difference is that the standards of what is allowable are different than at an academic center, etc.
Human Subject Issues • Medical Exception • Even though soldiers are consented to participate by higher authorities there are still extenuating circumstances • If a soldier has a medical contraindication to use a brace and is randomized to a “brace” group, then the soldier will not be forced to wear one • If a solider already has a medical necessity to wear a brace and is randomized to a “non-brace” group, then the soldier may keep the brace
Summary • Are ankle orthoses effective at reducing the risk of first ankle injuries in military recruits? • If YES, we can move forward with integrating their use during military high risk activities. • At this point, we would work with military officials and help with policy recommendations to implement the intervention.
References • M Schmidt, S Sulsky, and P Amoroso, “Effectiveness of an outside-the-boot ankle brace in reducing parachuting related ankle injuries,” Injury Prevention 11, no. 3 (June 2005): 163-168. • http://www.mmbrace.com/medspecbraces/anklebraces/aso-ankle-support1.htm • http://en.wikipedia.org/wiki/Incidence_%28epidemiology%29