Download
1 / 26
270 likes | 309 Views
Learn about macrocytic anemias, including megaloblastic and non-megaloblastic types, causes such as vitamin B12 and folic acid deficiencies, clinical features, lab diagnosis, treatment options, and bone marrow findings.

E N D
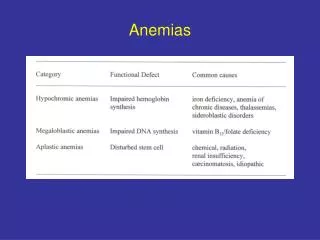
Macrocytic anemias • Macrocytic anemias are characterized by large RBCs with a normal hemoglobin content. • Macrocytic anemias are classified as • Megaloblastic • Non-megaloblastic
Megaloblastic anemias are associated with defective DNA synthesis leading to abnormal RBC maturation in the bone marrow (a nuclear maturation defect). • Megaloblastic anaemia is due to Vitamin B12 deficiency & folic acid deficiency
Megaloblasticanemias Primary defect in DNA replication is due to depletion of thymidine triphosphatewhich leads to retarded mitosis, and therefore retarded nuclear maturation. The depletion of thymidine triphosphate is usually due to a deficiency of vitamin B12 or folic acid. Cytoplasmic maturation proceeds ahead of nuclear maturation Nuclear/cytoplasmic asynchrony Granulocytic and megakaryocytic maturation are also affected leading to pancytopenia
Megaloblastic anemias • Vitamin B12 (cyanocobalamine) • Meats, eggs, dairy products, and liver. • Is absorbed in ileum via a binding protein called intrinsic factor (IF) • Folic acid (pteroyl glutamic acid) • Most foods, including eggs, milk, yeast, and liver. • Green, leafy vegetables and is synthesized by many microorganisms. • Is destroyed by heat • Absorption occurs in the duodenum & jejunum
CAUSES OF MEGALOBLASTIC ANEMIA • Vitamin B12 deficiency • Folic acid deficiency
Vitamin B12 deficiency A. Inadequate diet Eg: strict vegetarians, breast-fed infants B. Malabsorption 1. Gastric causes Pernicious anaemia, gastectomy, congenital lack of intrinsic factor 2. Intestinal causes Tropical sprue, ileal resection, Crohn’s disease
Folic acid deficiency A. Inadequate diet Poverty, elderly, alcoholics, teenagers, infants B. Malabsorption Tropical sprue, jejunal resection, Crohn’s disease, coeliac disease, partial gastrectomy C. Excess demand 1. Physiological: Pregnancy, lactation, infancy 2. Pathological : Malignancy, increased haematopoesis, tuberculosis, rheumatoid siseases D. Excess urinary folate loss Active liver disease, congestive cardiac failure
CLINICAL FEATURES Two categories • In both types of deficiency Pallor, weakness, lightheadedness Smooth red tongue Diarrhea alternating with constipation 2. In vitamin B12 deficiency only Neurological disturbances including Numbness and tingling of extremities Gait abnormalities Mental disturbances.
LAB DIAGNOSIS Hemoglobin and RBC counts are decreased Blood picture - Macrocytic anemia MCV=100-140 MCH is increased (due to increased cell size) MCHC is normal WBC and platelet counts are decreased Bone marrow – Megaloblasts Biochemical changes – rise in serun unconjugated bilirubin & LDH
Special tests • Serum vitamin B12 assay • Schilling test • Urinary excretion of FIGLU • Serum folate essay • Red cell folate essay
Peripheral smear • Triad commonly seen: 1. Oval macrocytes, 2. Howell Jolly bodies (nuclear DNA fragments) 3. Hypersegmented neutrophils (5 or more lobes). • In addition: • Anisocytosis is moderate • Poikilocytosis with nucleated RBCs, polychromatophilia, and cabot rings (spindle remnants). • RBC dimorphism is seen with concomitant IDA. • The absolute reticulocyte count is decreased because of ineffective erythropoiesis. • Progresses to pancytopenia
BONE MARROW PICTURE Hypercellular Megaloblasts Mega band forms Giant metamyelocytes Abnormal megakaryocytes with multilobated nuclei
SCHILLING TEST STAGE 1 – Hot Vit B 12 -0.5-2microgm (oral) Cold Vit B12-4mg (IV) Cold Vit B12-4mg saturates serum & tissue binding sites Normally more than 7% of 1 microgram of oral dose of hot Vit B12 is excreted Intrinsic factor deficiency - Reduced excretion STAGE 2 – if excretion is low then test is repeated with administration of intrinsic factor STAGE 3- repeat test after antibiotic dose
Pernicious anemia (PA) • 85% of megaloblastic anaemia is due to lack of intrinsic factor (IF) secondary to gastric atrophy – Pernicious anemia (PA) • Gastric atrophy is due to Autoimmune reaction against the gastric parietal cells in the G.I. tract. • Older adults (over 40). • Individuals of Northern European descent.
C/F • Anaemia • Glossitis • Neurologic manifestation • Diarrhea, wt loss • Hepatospleenomegaly Pathological changes • Gastric atrophy
Lab findings • Hypergastrinaemia • Blood & Bone marrow picture similar to megaloblastic anaemia • Schilling test abnormal • Rise in serum bilirubin, LDH, haptoglobin, ferritin & iron
Macrocytic anaemia -Non-megaloblastic • Haemolysis • Liver disease • Alcoholism • Hypothyroidism • Aplastic anaemia • Myeloproliferative disorders • Reticulocytosis