Download
1 / 38
380 likes | 534 Views
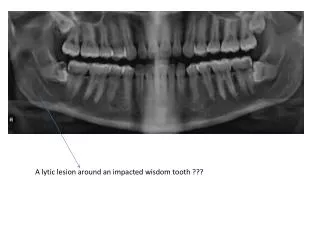
A pproach to imaging based diagnosis of an intracranial space-occupying lesion in a child. Dr. Flip Otto Dept Diagnostic Radiology UFS. Introduction. CNS tumours 2 nd most common after leukemia Incidence 2.4:100,000 children <15 years 15% of all paediatric neoplasms

E N D
Approach to imaging based diagnosis of an intracranial space-occupying lesion in a child Dr. Flip Otto Dept Diagnostic Radiology UFS
Introduction • CNS tumours 2nd most common after leukemia • Incidence 2.4:100,000 children <15 years • 15% of all paediatric neoplasms • 15-20% of all primary brain tumours • M>F • Usually presents with signs and symptoms of raised intracranial pressure and/or increasing head size
Approach – Clues to diagnosis • Age • Location • Local tumour spread • Solitary or multifocal • Specific imaging characteristics • Tumour mimics
Age • CNS tumours presenting at birth: • Teratoma (commonest) • Neuro-epithelial tumours: • Medulloblastoma • Astrocytomas • Ependymomas • Choroid plexus tumours • After 2 months, neuro-epithelial tumours more common. • During this time, supratentorial tumours more common than infratentorial
Age • Brain tumours in infants <2 years • Two thirds are supratentorial • Most common tumours: • PNET (primitive neuroectodermal tumour) • Astrocytoma • Teratoma • Choroid plexus papilloma
Most common CNS tumours in paediatric patients older than 2 years • Number of infratentorial tumours slightly exceeds supratentorial tumours • Medulloblastoma • Astrocytoma • Ependymoma • Craniopharyngioma • Gliomas • Metastases are rare in paediatric population (vs. 50% in adults)
Location • Intra- vs. extra-axial • Supra- vs. infra-tentorial • White matter vs. cortical based • Specific anatomic sites: • Sella/suprasellar • Pineal region • Intraventricular
Intra- vs. extra-axial • Signs of extra-axial location: • CSF cleft • Displaced subarachnoid blood vessels • Cortical grey matter between mass and white matter • Displacement and expansion of subarachnoid space • Broad dural base • Bony reaction • >80% extra-axial tumours are either meningioma or schwannoma
Intra-axial vs Extra-axial Brain Tumours Intra-axial Extra-axial Meningioma Pituatary adenoma Craniopharyngioma Schwannoma Chordoma Dermoid/epidermoid cyst Lipoma Metastases, hematoma, infection • Glioma • Medulloblastoma • Hemangioblastoma • Metastases • Infarction/hematoma • AVM • Abscess/inflammation
Supra- vs. infra-tentorial • Common intra-axial CNS tumours in paediatric age group • Supratentorial: • Astrocytoma • Pleomorphic xanthoastrocytoma • PNET • DNET • Ganglioglioma • Infratentorial: • Juvenile pilocytic astrocytoma • PNET (Medulloblastoma) • Ependymoma • Brainstem astrocytoma/glioma
White matter vs. cortical based • Most intra-axial tumours are white matter based • Differential diagnosis for cortical based tumours: • DNET (Dysembryoplasticneuroepithelial tumour) • Ganglioglioma
Specific anatomic sites • Sella/suprasellar: • Optic pathway/hypothalamic glioma • Craniopharyngioma • Germ cell tumours • Pineal region: • Germ cell tumours • Pinealblastoma (associated with retinoblastoma) • Astrocytoma • Ganglioglioma • Epidermoid • Intraventricular: • Ependymoma • Choroid plexus papilloma/carcinoma • Subependymal giant cell astrocytoma (associated with tuberous sclerosis ) • Lesions arising from suprasellar region may involve 3rd ventricle • Colloid cyst (3rd ventricle, usually young adults)
Intraventricular tumours: Choroid plexus papilloma and carcinoma
Local tumour spread • Astrocytomas spread along white matter tracts and don’t respect lobar boundaries • Ependymomas in 4th ventricle may extend through foramen of Magendie into cisterna magna, and through foramina of Luschka into cerebellopontine angles • Subarachnoid seeding: PNET; ependymomas; choroid plexus carcinoma
Mass effect • Primary brain tumours usually have less mass effect and oedema than expected for size, due to infiltrative growth pattern • Metastases and extra-axial tumours have more significant mass effect due to expansile growth pattern
Solitary vs. multifocal lesions • Metastases and CNS lymphoma, often presenting with multiple lesions, are rare in children • Seeding metastases may be seen with PNET-MB (Medulloblastoma) and ependymoma • Multiple brain tumours may occur in phacomatoses: • NF I: optic gliomas; astrocytomas • NF II: meningiomas; ependymomas; choroid plexus papillomas • Tuberous sclerosis: subependymal tubers; ependymomas; intraventricular giant cell astrocytomas • Von HippleLindau: hemangioblastomas
Specific imaging characteristics • Fat • Calcification • Cystic mass vs. cyst • T1WI signal intensity • T2WI signal intensity • Contrast enhancement • Advanced MRI
Fat • Fat is characterised by high signal on T1 and T2WI, with associated chemical shift artefact • Fat suppression sequences help distinguish from other causes of high signal e.g. melanin, hematoma and slow flow • Masses containing fat include teratoma, lipoma and dermoid cyst
Calcification • Intra-axial: • Astrocytoma • Ependymoma • Choroid plexus papilloma • Ganglioglioma • Extra-axial: • Meningioma • Craniopharyngioma
Cystic mass vs. cyst • Cystic lesions that may simulate tumours include epidermoid, dermoid, arachnoid, neurenteric and neuroglial cysts • To differentiate cystic masses from cysts: • Morphology • Fluid/fluid level • Content intensity compared to CSF on T1, T2 and FLAIR sequences • Restricted flow on DWI
T1WI signal intensity • Most brain tumours have low to intermediate signal intensity on T1WI • High T1 signal may be due to: • Methaemoglobin in a haemorrhagic tumour • High protein content egneurenteric cyst, dermoid cyst
T2WI signal intensity • Most brain tumours appear bright on T2WI due to high water content • Causes for low signal on T2: • Hypercellular tumours with high nuclear-cytoplasmic ratio : PNET, meningioma, germinoma • Calcifications • Hemosiderin in old haematomas • High protein content e.g. colloid cyst • Flow voids e.g. haemangioblastoma
Contrast enhancement • Extra-axial tumours, pituitary, pineal and choroid plexus tumours enhance (outside blood-brain barrier) • Contrast enhancement does not visualise full extent of infiltrative tumours eggliomas • In gliomas, enhancement indicates higher degree of malignancy • Ganglioglioma and pilocyticastrocytomas are exceptions, low grade tumours that enhance vividly
Contrast enhancement patterns • No enhancement: • Low grade astrocytoma • Cystic non-tumoral lesions • Homogeneous enhancement • Germinoma and other pineal tumours • Pituitary adenoma • Pilocytic astrocytoma(solid component) and haemangioblastoma • Ganglioglioma • Meningioma, schwannoma • Patchy enhancement • Radiation necrosis • Ring enhancement • High grade glioma • Metastases • Abscess
Advanced MRI techniques • Diffusion weighted imaging • Diffusion tensor imaging • Perfusion weighted imaging • Magnetic resonance spectroscopy
Application of Advanced MRI in Paediatric Brain Tumours • Improving the accuracy of the initial diagnosis • Evaluating the risk at initial diagnosis • Monitoring the effectiveness of therapy
DWI • Most tumours do not show significant restriction of diffusion • High signal on DWI is seen with abscesses, epidermoid cysts and acute infarction
PWI • Signal intensity depends on vascularity, not on breakdown of blood-brain barrier • Better correlation with grade of malignancy than degree of contrast enhancement
MRS • H-1 MRS analyzes signal of protons attached to other molecules • Output is collection of peaks at different radiofrequencies, representing proton nuclei in different chemical environments, proportional to number of contributing protons. • Peaks include: N-acetylaspartate; choline; creatine; myo-inositol; taurine; lactate; methyl groups(lipids); methylene groups
Tumour mimics • Abscesses can mimic metastases • Multiple sclerosis can present with mass like lesions with enhancement (tumefactive MS) • Aneurysms should always be excluded in the parasellar region
Conclusion • Primary CNS tumours relatively common in children • Age of child helps narrow differential diagnosis • Anatomical localization very important • CT and MRI findings characterize tumour composition • Advanced MRI techniques can aid in diagnosis, grading and monitoring treatment response
References • Daehnert, W. Radiology Review Manual 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. • Panigrahy, A., Blueml, S.(2009) Neuroimaging of Paediatric Brain Tumors: From Basic to Advanced Magnetic Resonance Imaging (MRI). Journal of Child Neurology.24(11),1342-1365. • Smithuis, R., Montanera, W. Brain Tumor - Systematic Approach. www.radiologyassistant.nl • Weisleder, R, Wittenberg, J, Harisinghani, MG, Chen, JW. Primer of Diagnosic Imaging 5th ed. St. Louis: Elsevier Mosby; 2011.