Download

1 / 11
110 likes | 127 Views
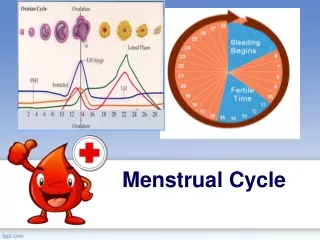
Uterine bleeding: either menstrual (normal) or abnormal uterine bleeding . Menstrual uterine bleeding (menses) : characterized by: 1. Bleeding from secretory endometrium. 2. There is ovulation. 3. Not exceeding a length of 5days .

E N D
Uterine bleeding:either menstrual (normal) or abnormal uterine bleeding. Menstrual uterine bleeding (menses): characterized by: 1. Bleeding from secretory endometrium. 2. There is ovulation. 3. Not exceeding a length of 5days. Any uterine bleeding not fulfilling these criteria is called abnormal uterine bleeding. Clinical terms used for disturbance of menstruation: 1. Menorrhagia (profuse or prolonged bleeding at the time of bleeding). 2. Metrorrhagia (irregular bleeding between the periods). 3. ovulatory (intermenstrual bleeding). Abnormal uterine bleeding: either of two types 1. Organic uterine bleeding (due to organic lesion in the uterus). 2. Dysfunctional uterine bleeding (bleeding
Causes of organic uterine bleeding: 1. Endometrial polyps. 2. Leiomyomas (specially subserosal 3. Endometriosis. 4. Endometritis. 5. Endometrial hyperplasia. 6. Endometrial carcinoma. 7. Cervical carcinoma. Dysfunctional uterine bleeding: causes: (1)Failure of ovulation: (anovulatory cycles) * commonest type. *Age: common at both ends of reproductive life. *Causes: 1. Dysfunction of hypothalamic pituitary axis. 2. Abnormality of adrenal or thyroid glands. 3. Functioning ovarian lesion producing excess of estrogen. 4. Malnutrition, obesity, debilitating dis. 5. Severe physical or emotional stress.
Pathogenesis:Whatever the cause, failure of ovulation---excess estrogen relative to progesterone---endometrium go through proliferative phase that is not followed by normal secretary phase. Mic: endometrial glands may develop mild cystic changes with relatively less stroma (absent progesterone), with rupture of spiral arterioles result in bleeding. (2) Ovulatory cycles:inadequate proliferative phase, or inadequate secretory phase (inadequate luteal phase), in both there is disparity between the endometrial pattern observed & that expected from the time of the cycle. (3)Contraceptive induced bleeding: Older pills contain synthetic estrogens----- endometrial responses (pseudodecidualization & inactive nonsecretory glands).
Endometrial hyperplasia(EH): Excess estrogen relative to progesterone if sufficiently prolong or marked induce endometrial hyperplasia. Classification of endometrial hyperplasia: 1. Simple endometrial hyperplasia (with or without atypia which is called atypical simple endometrial hyperplasia). 2. Complex endometrial hyperplasia (with or without atypia, called atypical complex endometrial hyperplasia). Causes: (1) Failure of ovulation around menopause. (2) Prolong administration of estrogen without counterbalance progesterone (3) Estrogen producing ovarian lesions e.g polycystic ovaries, granulosa &theca cc tumor of ovary.
Notes: Atypical EH shows 20-25% risk of progression to CA of endometrium . Tumors of endometrium &myometrium: Endometrial polyps: Gross: sessile ,hemispheric ,0.5-3 cm in diameter , the larger polyps may project from endometrial mucosa into uterine cavity. Mic:surface cover by columnar cell , some have adenomatous stroma with normal endometrial architecture or have cystically dilated glands similar to cystic hyperplasia. Age: more commonly at the time of menopause. Clinical importance: produce abnormal uterine bleeding & more important, the risk (however rare) of malignant transformation.
Leiomyoma(fibroid): * Benign tumors arise from smooth muscle cells in myometrium (fibroid). * the most common benign tumor in female & found in 30-50% during reproductive age, * More frequent in Blacks than Whites, * estrogen & OCC stimulate their growth & shrink in size post menaposly. * chromosomal abnormality is found in 40% of cases. Gross: Number: single or multiple (more common). Size:from small seedings to massive tumors. Color & texture: well circumscribed,firm, grey- white masses with characteristic whorled cut surface. Site: intramural leiomyoma (within myometrium). submucosal ==(beneath endometrium) subserosal == (below serosa) Parasitic == (subserosal leiomyoma may become separated from uterus & attached to the surrounding organs)
Secondary changes within the tumor: include Ischemic necrosis, hemorrhage, cystic changes, calcification (postmenapause). Mic: interlacing bundles of smooth muscles, foci of fibrosis, calcification & hemorrhage. Clinically: May be entirely asymptomatic &discovered on routine pelvic exam or postmortem. The most frequent manifestation is menorrhagia, large masses may become palpable to the patient or produce dragging sensation, extremely rare transform to sarcoma .
Leiomyosarcoma: Arise from mesenchymal cells of myometrium, not from preexisting leiomyoma. Gross: either 1. almost always solitary , bulky mass infiltrating uterine wall. 2. Polypoid masses projecting into uterine cavity. 3. Discrete tumors simulate large benign leiomyoma. Mic.:wide range of differentiation from closely resemble leiomyoma to widely anaplastic tumor, the diagnostic features are frequent mitosis with or without cellular atypia or less numerous mitosis with cellular atypia. Recurrence is common, may metastasize widely &40% 5 year survival
Endometrial carcinoma: *The most frequent cancer of the female genital tract. *Age incidence: 55-65years (uncommon below40) According to the pathogenesis, two types of endometrial carcinoma: Type I: endometroid carcinoma, those related to excess estrogen stimulation (commonest, about 80% of cases). Type II: those developing de novo (not related to the estrogen stimulation, form 20% of cases, oldage & poor prognosis) Risk factors for endometroid carcinoma : Obesity (increase synthesis of estrogen in fat depots). Diabetes milletus, Hypertension, infertility, Failure of ovulation (stein- leventhal syndrome) female tend to be single, nulliparas prolong estrogen replacement therapy Ovarian estrogen secreting tumors (granulosa cell tumor, thecoma). Breast cancer treated with tamoxifen. Severe endometrial hyperplasia.
Grossly: Either infiltrative cause diffuse thickening of uterine wall or exophytic mass. Histolog.: 80% of cases are adenocarcinom (endometroid carcinoma) (50% are well differentiated, 35% moderate, 15% Poor differentiated). FIGO STAGING System: Stage 0: Carcinomas in situ Stage I: Confined to the uterine corpus. Stage II: Tumor invade the cervix but not extend beyond uterus. Stage III: extend beyond uterus, but withion the pelvis. STAGE IV: distant metastases or involvement of other viscera. Clinically: marked leucorrhea &irregular bleeding reflecting erosion &ulceration of endometrial surface, with progression, uterus become enlarged & fixed to surrounding structures.