Download
1 / 20
200 likes | 456 Views
Gastro Intestinal Bleeding. By: Abdulrahman Sindi ED Resident. Case Scenario. A 55-year-old male not known to have any medical illness, presented to the E.D. complaining of blood in his vomitus two times this day. HR:120 BP:95/60 RR:22 T:36.7. Is the patient stable?

E N D
Gastro Intestinal Bleeding By: Abdulrahman Sindi ED Resident
Case Scenario • A 55-year-old male not known to have any medical illness, presented to the E.D. complaining of blood in his vomitus two times this day. • HR:120 • BP:95/60 • RR:22 • T:36.7
Is the patient stable? • What should be done for this patient? • What are initial steps in the management?
Epidemiology • GI bleeding is relatively common problem encountered in ED • The mortality rate is is approximately 10% • UGIB affects 50-150 people per 100,000 each year • Mean age of affected people with GIB is 59 years • UGIB is more common in men, whereas LGIB is more common in women • UGIB admission is more common in adults whereas LGIB admission is more common in children
Differential Considerations Adult Children • In children less than 2 years of age massive LGIB is most • often due to Meckels diverticulum or intussusception
Rapid Assessment and Stabilization • Patients with suspected GIB who are hemodynamically unstable should be stabilized and evaluated rapidly. • Undress and place cardiac and oxygen saturation monitors. • Give supplemental oxygen. • 2 large bore peripheral intravenous lines. • Take blood for (CBC, PT, type and screen or crossmatch). • Give bolus crystalloid. • Give type O, type specific or crossmatched blood. • Consult the GE in UGIB or surgeon in LGIB if persistently unstable.
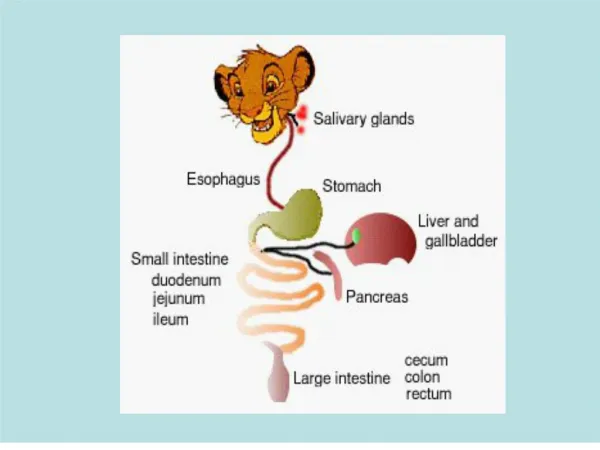
History • Hematemesis:: vomiting of blood that occurs in bleeding of the esophagus, stomach, or proximal bowel (50% in UGIB). • Melena: black tarry stool that results from the presence of 150-200 ml of blood for prolonged period (70% in UGIB and 33% in LGIB). • Hematochezia:
History • Hematemesis: vomiting of blood that occurs in bleeding of the esophagus, stomach, or proximal bowel (50% in UGIB). • Melena: black tarry stool that results from the presence of 150-200 ml of blood for prolonged period (70% in UGIB and 33% in LGIB). • Hematochezia: bright red blood in the stool that mostly occurs with LGIB but can occur in UGIB (66% in LGIB and 10-15% in UGIB).
History • Duration, quantity, associated symptoms, previous history, medications, alcohol, and associated medical illness
Physical Examination • Vitals: hypotension, tachycardia or postural change in heart rate. • General exam: general appearance, mental status, skin signs and abdominshould be assessed carefully. • Rectal exam: it’s the key to confirm the diagnosis, it does not exclude the diagnosis if negative
Ancillary Testing • Occult blood test: it may have positive result 14 days after a major bleed, it has a false positive and negative results, • Clinical labs: CBC, coagulation profile, type and screen and crossmatch • ECG: should be done to all patients over 50, preexisting cardiac insult, anemia, chest pain, S.O.B., persistent • Imaging: CXR if perforation is suspected
Management • Reassurance • N.G. tube and gastric lavage: • Aspiration of bloody content diagnoses UGIB, but it does not determine if it is ogoing • False negative results are possible if if bleeding is intermittent, in duodenal bleed, pyloric spasm. • False positive occurs in nasal bleeding. • The presence of bile in excludes the possibility of UGIB. • Gastric lavage is helpful to prepare for endoscopy • Lavage should not performed in pneumoperitoneum.
Management • Anoscopy/proctosigmoidoscopy. • Endoscopy: • It identifies lesion in 78% to 95% if done within 12 to 24 hours. • Angiography and tagged RBC scan: • Angiography is commonly used in LGIB • Detects 40% of LGIB site. • It is performed ideally in active bleeding. • In undetected bleeding tagged RBC scan is performed.
Management • Proton pump inhibitors • Octreotide • Vasopressin • Sengstaken-Blakmore Tube: • Stops bleeding in 80% of esophageal varices. • Indicated when endoscopy is not readily available and vasopressin has not slowed the bleeding. • Surgery: • Indicated in for all hemodynamically unstable with active bleeding unresponsive to resuscitation
Disposition • Very low criteria for GIB patients • No comorbid disease • Normal vitals • Negative guaiac test • Negative gastric aspiration • Normal hemoglobin/hematocrit • Proper understanding for signs and symptoms • Immediate access to ER • Arranged follow up within 24 hours
Thank You By Dr. Abdulrahman Sindi