Download

1 / 136
1.37k likes | 1.82k Views
Gastro- Intestinal System. Medication Administration. Digestive System. Food is vital for life as it is required for the chemical reactions that occur in every cell. The foods we eat are too large to pass through

E N D
Gastro- Intestinal System Medication Administration
Digestive System • Food is vital for life as it is required for the chemical reactions that occur in every cell. • The foods we eat are too large to pass through the cell’s membranes, therefore a thorough and extensive breaking down process must take place. This process is called digestion. Mechanical digestion consists of chewing, churning and peristalsis. Chemical digestion is performed by digestive enzymes. • The digestive system consists of the alimentary canal and the accessory organs
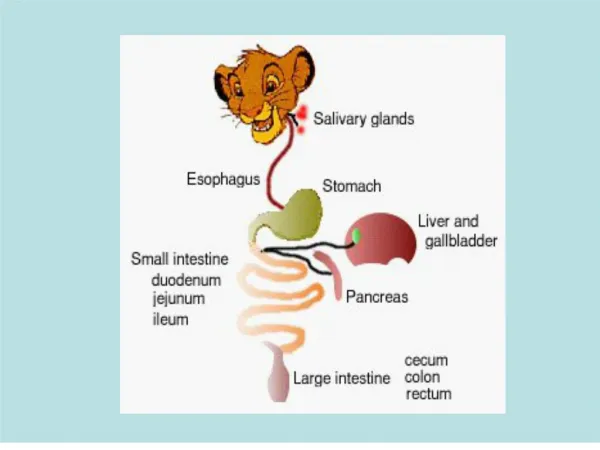
Digestive System • The Alimentary Canal • - is approx 27 feet long and extends from the mouth to the anus. • - is also referred to as the intestines, the gut or the digestive tract. • - consists of : the mouth • the pharynx • the oesophagus • the stomach • the small intestine • the large intestine • the rectum • the anal canal.
Digestive System • The GIT is under neural control. Receptors are found in smooth muscle and secretory cells. SNS has inhibitory effect, PSNS via the Vagus, has exhitatory effect. • The organs of the abdomen are covered by serous membranes called the peritoneum. The visceral peritoneum covers the organs, the parietal peritoneum lines the abdominal wall. • The peritoneal cavity is filled with a lubricating fluid secreted by the membranes. An increase in this fluid is called ascites. • The layers of the peritoneum are connected by the mesentery. The mesentery also allows nerves, blood supply and lymph vessels to reach the digestive organs. Greater omentum and lesser omentum.
The Digestive Process • 1. Ingestion ; the taking in of food into the body • 2. Secretion ; of various protective and digestion fluids. • 3. Peristalsis ; the movement of food along the digestive tract. • 4. Digestion ; the breakdown of food by both mechanical and chemical processes. • 5. Absorption ; the passage of digested food from the digestive tract into the cardiovascular and lymphatic systems for distribution to cells. • 6. Defecation ; the elimination of indigestible substances from the body.
Digestive System • THE MOUTH • Food is ingested through the mouth into the bucchal cavity, where it is broken down with the help of saliva. • Salivary amylase acts to break down carbohydrates and this is the first step in digestion. Lingual lipase acts to break down fats. • Saliva also moistens food, helps it form a bolus and keeps the mouth clean. • Salivation is regulated by the PSNS. The SNS inhibits saliva excretion. • There are 3 pairs of salivary glands – sublingual, submandibular and parotid.
Digestive System • THE PHARYNX AND EPIGLOTTIS • THE OESOPHAGUS • Once food particles are moistened, they move into the oesophagus. The oesophagus is approx. 25cm long and is usually in a collapsed state unless food is present. It is a muscular structure, which performs peristaltic waves to move food along. • The entrance to the stomach is protected by the cardiac sphincter, or the gastro-oesophageal sphincter. This is essential to prevent reflux backwards.
Digestive System • THE STOMACH • The bolus of food moves by peristalsis through the oesophagus into the stomach. • The stomach is a J – shaped pouch which is divided into the cardiac region, the fundus, the body and the pylorus. • The entrance into the small intestine is protected by the pyloric sphincter, which regulates emptying.
Digestive System • The lining of the stomach contains : • Goblet cells - which produce large amounts of protective mucus. • Parietal cells - produce hydrochloric acid and intrinsic factor. Secretes 1 – 2 litres of HCl per day HCl kills bacteria and activates pepsin s protein. • Intrinsic factor is a small • protein required for Vit B12 to be absorbed in the ileum • of the small intestine. Vitamin B12 is required for the • maturation of erythrocytes ( pernicious anaemia exists when • there is a lack of intrinsic factor)
Digestive System • - have Histamine (H2) receptors. Histamine promotes acid • secretion, prostaglandins inhibit acid secretion • Chief cells – produce pepsinogen which is the inactive form of pepsin. • Enteroendocrine cells – release gastrin, a hormone which stimulates • stomach secretion and mobility. Also releases • cholecystokinin, serotonin, histamine, somatostatin • and endorphins. • Therefore, gastrin, acetylcholine and histamine all directly stimulate receptors to increase acid secretion by parietal cells. • The lining of the stomach is thrown into folds called rugae, to increase it’s surface area. Holds up to 2 litres of content.
Digestive System • The stomach walls have three layers of smooth muscle – longitudinal, circular and oblique. These mix and churn the contents, as well as assisting with emptying. • At the end of the process, the food has been reduced to a paste or a liquid form that we refer to as chyme. • Chyme passes through the duodenal sphincter, into the duodenum and it’s presence stimulates enzyme release. • It also stimulates the inhibition of gastric activity.
Digestive System • THE SMALL INTESTINE • The small intestine is divided into the duodenum, the jejunum, the ileum and joins the large intestine at the ileocaecal valve. • It is approx. 7m long, has convolutions and internal villi to increase it’s absorptive surface area. • Intestinal juice is alkaline and contains water, mucus and where most of the digestion and absorption processes occur. • Peristalsis moves the chyme along. This is the series of contraction and relaxation of the muscular wall of the intestine. This is under involuntary control.
Digestive System • Segmentation also occurs, but it’s main purpose is to mix the contents with intestinal juices and mechanically breaks down contents. • Bile acts to break down fats and then these fats are absorbed by the lacteals of the lymphatic system. • Different enzymes come into play, to release the nutrients. Pancreatic enzymes act on sugars, starch, fats and protein which are then absorbed into the bloodstream through the intestinal wall. • It is the principle site of drug absorption.
Digestive System • THE LARGE INTESTINE • The large intestine’s function is to propel the contents towards expulsion and to also absorb water from the contents of it’s lumen. The lining changes to columnar epithelium with goblet cells, which offers greater protection. • Mucus protects the bowel wall. • Bacteria present in the bowel act on it’s contents, as deodorizers, and they also produce vitamins K and B complex. • The cecum is the first section. The appendix is attached here, which is a mass of lymphoid tissue.
Digestive System • The cecum leads into the ascending colon, turns at the hepatic flexure, becomes the transverse colon, turns again at the splenic flexure, and then becomes the descending colon. • It then becomes the sigmoid colon at the level of the pelvis. • Progressively it becomes the rectum and terminates as the anal canal and anus. • The presence of faecal material entering the anal canal, stimulates nerve endings and sends messages to the brain. The PSNS causes the sigmoid colon and rectal walls to contract, and the external voluntary anal sphincter to relax. • This results in defaecation. Decomposition of bilirubin contributes to the colour of faeces.
Digestive System • The Accessory Organs • - include : the teeth • the tongue • the salivary glands • the liver • the gallbladder • the pancreas.
Digestive System • THE LIVER • The liver is the body’s largest gland. It is divided into 2 lobes, and then these 2 lobes are further divided into specialized cells called hepatocytes. • The liver doesn’t have capillaries. Instead it’s hepatocytes are arranged into a series of canals which blood flows through. Toxins and nutrients are removed as they flow through these canals. • Produces bile to aid in the digestion of fats. This bile leaves the liver via the hepatic duct and then joins with the cystic duct to form the common bile duct. This then empties into the duodenum.
Digestive System • Bile is an alkaline liquid containing bile salts, cholesterol, pigments - bilirubin, fats, phospholipids and electrolytes. It emulsifies fats. • The liver has a metabolic role; to process the mass of nutrients delivered to it from blood from the intestine. • Group work • Divide into pairs or small groups. • Refer to page 532 of Bryant. • List the various metabolic roles of the liver.
Digestive System • THE GALLBLADDER • Is a small, muscular organ which functions to store and concentrate bile. • Cholecystokinin is a hormone secreted by the cells of the duodenum, in response to the presence of food. It’s role is to stimulate the contraction of the gallbladder, to eject bile into the lumen of the S.I.
Digestive System • THE PANCREAS • Produces many digestive enzymes which leave the pancreas via the pancreatic duct. This also joins with the common bile duct, and empties into the duodenum. It secretes up to 1500mls of fluid per day. • Islets of Langerhans release insulin and glucagon. Glucagon is responsible for glycogen breakdown in the liver. • Acinar cells release digestive enzymes - Proteases which digests proteins • Amylase which digests carbohydrates.
Digestive System • Lipase which digests fats. • Nuclease which digests nucleic acids. • Pancreatic duct cells produce bicarbonate. This neutralizes the chime. • Produces trypsinogen, the inactive form of trypsin which digests proteins. • Produces Chymotrypsinogen, the inactive form of chymotrypsin which also digests proteins.
Digestive System • FOOD SOURCES • Glucose : carbohydrates, sugars. • Amino acids : protein, fish, chicken, meat, pulses. • Vitamins : Fat soluble ; A, D, E, K, • Water soluble ; B Group, C, Folic Acid, • Minerals : Calcium, Magnesium, Iron, Potassium, Sodium.
Digestive System • DISEASES AFFECTING THE G.I. TRACT • Oral Candidiasis • A fungal infection of the mouth with candida albicans - also known as thrush. • Causes : reduced immunity, smoking, reduced salivation, oral trauma, • S & S : painful, sore mouth, dysphagia, reddened oral mucous membranes, whitish – grey plaques present in mouth – on tongue, inner cheek, soft palate, etc. • Treatment : oral hygiene – mouth rinses, clean teeth • : medications – anti fungal agents • Please research Nystatin, and Miconazole
Digestive System • Herpes Simplex • A viral infection with varicella zoster affecting lip surfaces – also known as cold sores. • S & S : lesions usually affecting the edges of lip surfaces. Progress from redness, to • pustule, to crusted lesion. • Treatment : rest, nutrition, fluids, • : medications - anti pyretics, • - antivirals • Please research Zovirax
Digestive System • Oesophagitis • Often referred to as heartburn. • Caused by the refluxing of acidic gastric contents up into the oesophagus. • List some common causes of reflux ; • Treatment ; variable depending on the cause. Often use antacids to neutralize the acidity. • Antacids consist of sodium bicarbonate, or aluminium hydroxide, • Refer to pg 538 of Bryant. • Choose 1 antacid and list it’s composition, action, side effects and drug interactions.
Digestive System • Gastritis / Gastric Ulceration • Inflammatory processes that cause weakening and breakage the protective lining of the stomach. • Causes : NSAIDs, alcohol, smoking, stress, bacteria, reduction in protective mucus, mucosal ischaemia.. • Complications : gastric bleeding, iron deficiency anaemia, perforation, • haemorrhage, pernicious anaemia.
Digestive System • S & S : nausea, epigastric pain, abdominal pain, S & S of anaemia, acute G.I. blood loss, etc • Treatment : medications – reduce acidity, by use of antacids such as sodium • bicarbonate or aluminium hydroxide.. • - reduce production of gastric acid – PPI, H2 antagonists • - increase protective lining – cytoprotective agents • - antibiotics, • life changes - reduce alcohol intake, stop smoking, stress reduction
Digestive System • Helicobacter pylori is a spiral-shaped, gram negative bacteria. It is able to change urea in the stomach into ammonia and bicarbonate, to protect itself from the acidity of the gastric secretions. • Group research • In pairs or small groups, • Research Triple Therapy. • Losec HP7 or Klacid HP • What are the contents of these medications? • How do they have their effect?
Digestive System • Duodenal Ulceration • More common than gastric, and again occurs when inflammatory processes disrupt the lining of the duodenum. • Causes : over secretion of acid and over secretion of pepsin. • Helicobacter Pylori. • Complications : bleeding, rupture,
Digestive System • S & S : abdominal pain, anaemia, darkened stool, • Treatment : medication – PPI, H2 Antagonists • Proton Pump Inhibitors, or PPIs, suppress gastric acid secretion by inhibiting the Hydrogen – Potassium Adenosine Triphosphatase (ATPase) enzyme system at the secretory surface of the gastric parietal cells. By this action they block acid production. Eg Omeprazole. • Research one of the following – Omeprazole • - Lansoprazole • - Pantoprazole • - Rabeprazole • - Esomeprazole
Digestive System • Histamine Receptor Antagonists work by blocking the effect of histamine on the parietal cells. Histamine (H2) increases acid production. • Research one of the following – Cimetidine • - Ranitidine • - Famotidine • - Nizatidine • Cytoprotective agents provide a physical barrier. • Research one of the following – Sucralfate • - Misoprostol
Digestive System • Vomiting • Caused by stimulation of the emetic centre which is found in the medulla of the brain. • Stimulants : the chemoreceptor trigger zone(CTZ) of the brain ( which is stimulated • by toxic substances in the blood, and also by the following areas.) • - the vestibular apparatus. • - areas of the heart, and GI tract • - the brain itself – smell, pain, sight.
Digestive System • The chemoreceptor centre stimulates the emetic centre by means of neurotransmitters – serotonin, acetylcholine, histamine and dopamine. • The emetic centre stimulates contraction of abdominal muscles and diaphragm to increase intra abdominal pressure. This forces contents up and out. • There is also stimulation of the SNS and PSNS which accounts for the associated salivation, pallor, diaphoresis, nausea and heart rate changes. • Most anti emetics target the neurotransmitters.( p 540 ) They block their effect in either the emetic centre, the CTZ, the vestibular apparatus or the cerebral cortex.
Digestive System • Group 1 ; research Droperidol • Group 2 ; research Metoclopramide • Group 3 ; research Prochloperazine • Group 4 ; research Haloperidol • Group 5 ; research Ondansetron • Group 6 ; research Promethazine • Group 7 ; research Domperidone
Digestive System • Other drugs can also be used – dexamethasone, methylprednisolone, • benzodiazepines. • How do corticosteroids work as anti emetics? • Natural therapy - ginger
Digestive System • DIARRHEOA • The frequent passing of fluid faecal material. • Causes : increased peristaltic activity – toxins, • : presence of material that is unable to be reabsorbed. • : increased secretions by the SI or LI • Treatment : Adsorbents or opioids • Give an example of each
Digestive System • CONSTIPATION • The infrequent passing of hard faecal material. • Causes : dehydration, poor fibre intact, medications, disease, obstruction. • Treatment : Laxatives • Bulk forming • Faecal Softeners • Stimulant • Osmotic • Saline • Give an example of each
CSHALDERS/GOTAFE/2008 Emetic and Antiemetic Agents By Clare sahlders/GoTafe/2007
CSHALDERS/GOTAFE/2008 Managing Nausea and Vomiting • Emetics • Cause vomiting • No longer recommended for at-home poison control • Antiemetic • Decrease or prevent nausea and vomiting • Centrally acting or locally acting • Varying degrees of effectiveness
Sites of Action of Emetics/Antiemetics CSHALDERS/GOTAFE/2008
CSHALDERS/GOTAFE/2008 Focus on the Antiemetic Prototype: Prochlorperazine (Compazine • Indications:Control of severe nausea and vomiting due to causes such as migraine and vertigo • Adverse effects: constipation,dry mouth,sleepiness, dizziness, blurred vision. • Actions:Mechanism of action not understood; depresses various areas of the CNS • Routes: Oral, PR, IM, IV • Unknown; metabolized in the liver and excreted in urine
CSHALDERS/GOTAFE/2008 Focus on the Nonphenothiazine Antiemetic Prototype: Metoclopramide (Reglan) • Indications:Prevention of nausea and vomiting associated with emetogenic cancer chemotherapy; prevention of postoperative nausea and vomiting, opiod medications • Actions: Blocks dopamine receptors and accelerated gastric emptying, reduces refluxenhances motility og the upper GI tract • Routes: Oral, IM, IV • 5–6 hr; metabolized in the liver and excreted in urine
CSHALDERS/GOTAFE/2008 Metoclopramide • Pharmokinetics: Peak plasma conc occur 30-180 mins after oral administration, 10-15 mins after IM dose and within 5-20 mins after IV • Half life 2.5-5 hours • CNS depressant effect with a combination of metoclopramide and CNS depressant drug. • Adverse effects: diarrhoea, sleepiness, restlessness, dizziness, headache, hypotension, taccycardia • Caution: In parkinsons disease and depression can worsen symptoms • Dosage: Oral 10mg QID
CSHALDERS/GOTAFE/2008 Anticholinergics/Muscarinic Receptor Antagonists • Types • Hyoscine (scopolamine) • Action • Action of acetylcholine at muscarinic receptors and is used to prevent motion induces nausea and vomiting by depressing conduction in the labyrinth of the inner ear • Adverse effects: Dry mouth, taccy, blurred vision, const, mental conf, fatigue and restlessness • Admin: 30 mins prior to travel eg. Travacalm
CSHALDERS/GOTAFE/2008 5-HT3 Receptor Blockers • Action • Block those receptors associated with nausea and vomiting in the CTZ (chemoreceptor trigger zone) and locally • Types • Dolasetron (Anzemet), tropisetron, ondansetron (Zofran), and palonosetron (Aloxi) • Pharmacokinetics • Rapidly absorbed, metabolized in the liver, and excreted in urine and feces
CSHALDERS/GOTAFE/2008 Focus on the 5-HT3 Receptor Blockers Prototype: Ondansetron • Indications:Control of severe nausea and vomiting associated with emetogenic cancer chemotherapy, radiation therapy; treatment of postoperative nausea and vomiting • Actions:Blocks specific receptor sites associated with nausea and vomiting, peripherally and in the CTZ • Oral route: Onset 30–60 min; duration 1.7–2.2 h • IV route: Onset immediate; duration infusion time • :3.5–6 h; metabolized in liver; excreted in urine
CSHALDERS/GOTAFE/2008 5- HT 3 Receptor Antagonist/ Ondansetron • Ondansetron first used in nausea and vomiting assoc with cytotoxic agents and radiotherapy • Pharmakinetics: Max 1-1.5 hrs and plasma half life is 3-4 hours. Met in liver Less than 10% excreted unchanges in urine • Adverse effects: constipation, headache, anxiety and dizziness • Caution: In patients with liver damage • Dosage: Oral 8mg thirty mins before chemo then 4-8mg every 12 hours for 1-2 days
CSHALDERS/GOTAFE/2008 Indications for Antiemetics • Phenothiazines • Nausea and vomiting, including that associated with anesthesia; severe vomiting; intractable hiccoughs • Anticholinergics • Nausea and vomiting associated with motion sickness or vestibular (inner ear) problems • 5-HT3 receptor blockers/substance P/neurokinin 1 receptor antagonists • Nausea and vomiting with emetogenic chemotherapy
CSHALDERS/GOTAFE/2008 Contraindications to Use of Substance P/ Neurokinin 1 Receptor Antagonists • History of allergy to antiemetic • Impaired renal or hepatic function • Pregnancy or lactation • Coma or semiconscious state • CNS depression • Hypotension or hypertension • Active peptic ulcer • CNS injury
CSHALDERS/GOTAFE/2008 Antacids • Chemical compounds that neutralise hydrochloric acid in the stomach and thereby increase gastric PH • Ingredient: aluminium hydroxide, calcium carbonate, magnesium salts and sodium bicarbonate • Dexsal, Gastrogel, Gaviscon, Mylanta, Quick Eze • Dosage: Varies to individual. Fasting effects lasts 20-40 mins. 1 hour after meal effects up to 3 hours. • Liquid and powder from more effective