Download
1 / 20
230 likes | 698 Views
DISEASES OF THE HEART. K.V.BHARATHI. Agenda:. Normal heart. Heart failure. Congenital heart disease. Ischemic heart disease. Sudden cardiac death. Hypertensive heart disease. Valvular heart disease. Cardiomyopathies. Pericardial disease. Tumors of the heart. Cardiac transplantation.

E N D
DISEASES OF THE HEART K.V.BHARATHI
Agenda: • Normal heart. • Heart failure. • Congenital heart disease. • Ischemic heart disease. • Sudden cardiac death. • Hypertensive heart disease. • Valvular heart disease. • Cardiomyopathies. • Pericardial disease. • Tumors of the heart. • Cardiac transplantation.
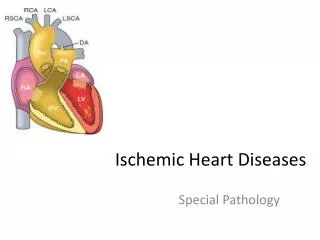
The normal heart: • Weight:Approximately 250-300g in female,300-350g in male. • RV free wall thickness:0.3-0.5 cm. • LV free wall thickness:1.3-1.5 cm. • Blood Supply:The coronary arteries--- • Left anterior descending(LAD)supplies most of the apex,the anterior wall of LV & anterior 2/3rds of the IVS. • Left circumflex(LCx) supplies LV myocardium. • Right coronary artery(RCA) supplies RV free wall & posterior 1/3rd of the IVS.
Pathology • Failure of the pump-due to weak contraction OR insufficient relaxation. • Obstruction to flow-valvular lesions or lesions that cause outflow obstruction. • Regurgitant flow-incompetent valves,dilated heart. • Disorders of cardiac conduction-heart blocks & arrhythmias. • Disruption of circulatory system continuity-dissection,trauma.
Cardiac failure • End result of many pathological processes • Leads to complex adaptive processes • Increased sympathetic tone • Antidiuretic hormone secretion • Increased renin-angiotensin activity • Increased cardiac muscle bulk
Causes of cardiac failure • Hypertension • Valve disease • Lung disease • Ischaemic heart disease • Cardiomyopathy
Right and left heart failure • Interrelated but can be distinct especially in early stages. • Left – pulmonary congestion/oedema. • Right – systemic congestion ( jugulovenous pressure), hepatomegaly. • “Congestive cardiac failure” (CCF) – both sides of the heart show features of failure.
Cardiac output • Usually decreased in cardiac failure • High output failure caused by: • Increased blood volume. • Anaemia (severe). • Cirrhosis (vasodilatation with decreased peripheral resistance). • “Wet” Beri-beri.
Cardiac hypertrophy:pathophysiology & progression to failure • Cardiac myocyte can hypertrophy but not undergo hyperplasia. • Increased mechanical load causes hypertrophy. • Can weigh upto 400-800 g (2-3 times of normal). • Causes: • Systemic hypertension. • AS & AR. • MR. • Dilated / hypertrophic cardiomyopathy.
Pattern of hypertrophy reflects the nature of the stimulus! • Pressure-overloaded ventricles show concentric hypertyrophy as in Hypertension & AS. • LV shows increase in wall thickness with reduced cavity diameter. • Volume-overload causes eccentric hypertrophy with an increase in both wall thickness & cavity diameter due to LV dilatation. • The causes are MR,AR ,dilated cardiomyopathy. • Cardiac dysfunction follows both these types of hypertrophy.
Morphology of left-sided failure: • Heart—Non-specific changes of hypertrophy & fibrosis in the myocardium.The LA may be dilated & may contain thrombus. • Lungs—Pulmonary congestion with perivascular & interstitial transudate,accumulation of oedema fluid in alveoli,hemosiderophages or “heart failure cells”. • Kidneys—Decreased cardiac output causes a decrease in renal perfusion.This activates the Renin-Angotensin-Aldosterone system,which causes salt & water retention. • Persisiting perfusion deficit can cause Pre-renal azotemia. • Brain—Cerebral hypoxia with hypoxic encephalopathy.
Morphology of right-sided failure: • Usually a secondary consequence of left-sided failure. • Pure right-sided failure occurs with chronic severe pulmonary hypertension:cor-pulmonale. • Liver & Portal system—congestive hepatomegaly with passive congestion. • With long standing severe right-sided failure, central areas of the hepatic lobule show fibrosis along with necrosis,creating so-called cardiac sclerosis or cardiac cirrhosis. • Elevated portal pressure can cause congestive splenomegaly,with marked sinusoidal congestion. • Transudate in the peritoneal cavity---Ascites. • Kidneys---Show congestion & can lead to Azotemia. • Brain---identical to left-sided failure. • Pleural & pericardial effusion. • Subcutaneous tissues---dependant edema, can lead to generalized massive oedema:Anasarca.
Pathological changes • As for causative condition + ventricular hypertrophy/dilatation. • Pleural effusion. • “Nutmeg” liver:Cardiac cirrhosis/sclerosis of liver.