Download

1 / 23
230 likes | 247 Views
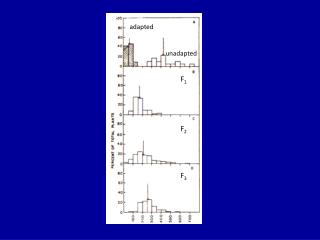
Risk Adapted Therapy for ALL. 서울아산병원 내과 이 제 환. Event-free survival. Overall survival. St. Jude Children’s Research Hospital, 2255 children with ALL, 1962-1997. (Pui CH et al, N Engl J Med 1998;339:605 ). St. Jude Children’s Research Hospital, 1984-1997.

E N D
Risk Adapted Therapy for ALL 서울아산병원 내과 이 제 환
Event-free survival Overall survival St. Jude Children’s Research Hospital, 2255 children with ALL, 1962-1997 (Pui CH et al, N Engl J Med 1998;339:605)
St. Jude Children’s Research Hospital, 1984-1997 (Pui CH et al, N Engl J Med 1998;339:605)
Cytogenetic Abnormalities in ALL (Faderl S et al, Cancer 2003;98:1337)
Immunologic Classification of ALL German Multicenter Study Group for Adult ALL (GMALL) (Ludwig WD et al, Leuk Lymphoma 1996;13:71)
Cytogenetic Abnormalities in ALL (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Cytogenetic Abnormalities in ALL • 51-65 chromosomes • Chromosomes 4, 6, 10, 14, 17, 18, 21, X • Low incidence in adult ALL • ? Prognosis in ALL • gain in chrom 4, 6, 10, 17: good prognosis • gain in chrom 5, isochrom 17, I(17)(q10): poor prognosis (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Cytogenetic Abnormalities in ALL • 45 chromosomes or less • 45 chromosomes (ex, monosomy 7): • most frequent, intermediate prognosis • 33-44 chromosomes: • rare (0.8%) • poorer outcome than 45 chromosome (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Cytogenetic Abnormalities in ALL t(9;22)(q34;q11) BCR/ABL hybrid gene 20-30% of all adult ALL cases > 50% in older patients > 55 yrs Almost exclusively found in B-precursor ALL (c-ALL/pre-B-ALL) Most unfavorable prognostic subgroup (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Cytogenetic Abnormalities in ALL t(4;11)(q21;q23) ALL1-AF4 (MLL-AF4) hybrid gene 5% of all adult ALL cases assoc. with pro-B-ALL (CD10 negative) > 50% in pro-B-ALL Poor prognosis (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Cytogenetic Abnormalities in ALL t(10;14)(p15;q11) TCR gene on chromosome 14 t(11;14)(p15;q11), t(11;14)(p13;q11) T-ALL Better outcome (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Cytogenetic Abnormalities in ALL p15, p16 genes CDK4, CDK6 40% Prognostic value: unclear (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Targets for Detection of MRD (Foa R et al, Rev Clin Exp Hematol 2002;6:181)
Results of Multicenter Studies in Adult ALL (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Treatment of Adult ALL • Induction chemotherapy • CR: at least 80% • Good remission quality: MRD below 10-3 to 10 -4 after induction • Dexamethasone (vs. prednisone), cyclophosphamide, anthracycline (dose intensity and schedule), L-asparaginase (native E.coli, Erwinia, PEG), high-dose cytarabine • Prophylactic use of growth factors • Consolidation therapy • Early and late intensification • High dose methotrexate, high dose cytarabine • Maintenance therapy • Hematopoietic cell transplantation • Allogeneic vs. autologous • CNS prophylaxis • CNS irradiation
HCT Indications in Adult ALL (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Monoclonal Antibody Therapy in ALL (Hoelzer D et al, Hematology 2002;162)
Risk Stratification of Adult ALL • Risk stratification models by prognostic factors • Identification of patients that are candidates for HCT in first CR • Characterization of biologic subgroups • Improvement with subgroup adjusted therapy treatment schedules • ALL is not a uniform disease. • Subtypes with distinct biologic, clinical, and prognostic features. • Clinical features: WBC, immunophenotype, cytogeneitc and molecular aberrations, time to CR, course of MRD • Leukemia-free survival according to subtypes
Immunophenotypic Subgroup of Adult ALL (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Immunophenotypic Subgroup of Adult ALL (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Risk Classification in Adult ALL (Gökbuget N et al, Rev Clin Exp Hematol 2002;6:114)
Summary • Risk adapted therapy • Risk adapted therapy in adult ALL has already resulted in major improvements in treatment outcome of B- and T-ALL. • Future perspectives • Specific treatment elements • T-ALL: cyclophosphamide, cytarabine, T-cell specific drugs • Pro-B-ALL: high dose cytarabine • B-precursor ALL: high dose cytarabine, 6-mercaptopurine • Mature B-ALL: high dose methotrexate, high dose cytarabine • Post-remission therapy intensity and duration • Should be adapted to risk of relapse • Hematopoietic cell transplantation • Indication for allogeneic HCT in first CR • Indication for matched unrelated HCT • New modalities for HCT: nonmyeloablative HCT, better conditioning • Evaluation of MRD • Immunotherapy: monoclonal antibody • Targeted therapy: imatinib mesylate