Download
1 / 36
360 likes | 438 Views
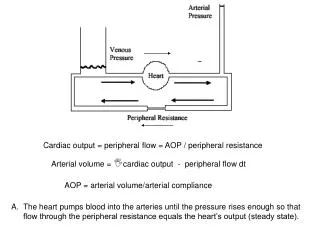
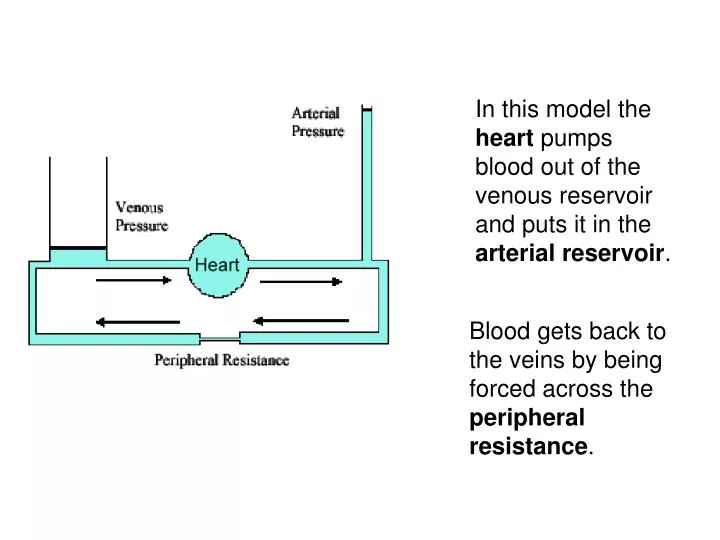
In this model the heart pumps blood out of the venous reservoir and puts it in the arterial reservoir. Blood gets back to the veins by being forced across the peripheral resistance. ΔP = R•CO. ΔP. Flow =. R.

E N D
In this model the heart pumps blood out of the venous reservoir and puts it in the arterial reservoir. Blood gets back to the veins by being forced across the peripheral resistance.
ΔP = R•CO ΔP Flow = R Blood will accumulate in the arterial reservoir until the pressure is high enough to push blood across the peripheral resistance at the same rate as the cardiac output.
A change in pressure in a compartment must be due to a change in volume. Since there is a fixed amount of blood in the system any rise in volume on one side must be at the expense of volume on the other side.
The arterial reservoir has less compliance than the venous side. Thus a large change in arterial pressure causes a much smaller change in venous pressure
The venous pressure is the filling pressure for the heart (a primary determinant of stroke volume)
A rat is sacrificed and half of class studies his heart while the other half study the vascular system by replacing the heart with an electric pump
The half with the heart rediscovers the ventricular function curve: They find that cardiac output is determined by LVEDP
The other half finds that both arterial and venous pressure vary as a function of cardiac output. • At zero cardiac output venous and arterial pressure are the same. • When the pump is started the two pressures separate.
It is noted that both graphs have the same axis Venous pressure = LVEDP
Take the vascular curve and swap the axes so pressure is on the horizontal.
The pressure at zero cardiac output is called mean systemic filling pressure. Expand the pressure scale and throw away the arterial curve. venous pressure curve
If we connect the heart on the right to the blood vessels on the left what would the cardiac output be?
The solution is a simple simultaneous equation that can be solved graphically by co-plotting the curves. There is only one cardiac output that can satisfy both systems. The crossing point determines that cardiac output.
If contractility is increased (e.g. sympathetic nerve stimulation) then cardiac output will rise and venous pressure will fall.
If contractility is decreased then cardiac output will fall and venous pressure will rise. Heart Failure This is part of the reason venous pressure rises in CHF
If total blood volume (TBV) is increased the venous pressure curve will be shifted up in a parallel fashion ΔP = R•CO Cardiac Output Venous Pressure
Decreased blood volume (hypovolemia) will cause a parallel shift of the venous curve down. Increased blood volume (hypervolemia) will cause shift in the curve upwards.
Loss of blood (hypovolemia) reduces cardiac output and venous pressure. If blood loss is large nothing will restore cardiac output except volume replacement It’s the low filling pressure that reduces the cardiac output. hemorrhagic shock The venous pressure distinguishes low contractility from hypovolemia
Changing venous tone has the same effect as changing blood volume, a parallel shift in the venous pressure curve. Increased Venous Tone Decreased Venous Tone The lower curve shows venodilation where venous compliance (VC) is increased. While the upper curve is a venoconstriction.
Increased Venous Tone Constricting the veins increases venous pressure and cardiac output. Venoconstriction is a common way for the body to increase its cardiac output
Decreasing the peripheral resistance causes a clockwise rotation of the venous pressure curve around the x axis intercept.
At zero flow increasing resistance has no effect on venous pressure When the heart is pumping increasing resistance will raise arterial pressure and lower venous pressure Thus the rotation around mean systemic filling pressure.
But wait, there’s more Decreased peripheral resistance by itself would increases filling pressure and increase cardiac output
Because the aortic pressure will fall, the heart will have an increased stroke volume for any filling pressure.
That will further increase cardiac output but will tend to lower venous pressure Because the aortic pressure will fall, the heart will have an increased stroke volume for any filling pressure.
An increased peripheral resistance will lower cardiac output. The overall effect on venous pressure is therefore ambiguous.
Thankfully, these are the only 4 maneuvers the body can use to alter the cardiac output!
Stroke volume Is determined by Aortic & venous pressure 1 contractility Three levels of Cardiac output regulation Is determined by Interactions between the heart and the vasculature 2 Is determined by CNS and hormonal control systems 3
The sympathetic nervous system cannot separately constrict the arterioles separate from the small veins. Yet arteriolar constriction reduces cardiac output while venous constriction increases it. What is the body trying to accomplish?
What would the control for activating the sympathetic nerves be labeled?