Download
1 / 1
10 likes | 110 Views
Racial and Ethnic Differences in Cardiac Resynchronization Therapy Outside of Published Guidelines.

E N D
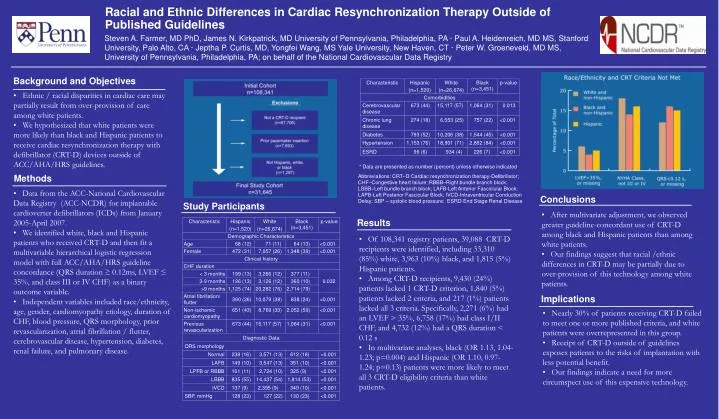
Racial and Ethnic Differences in Cardiac Resynchronization Therapy Outside of Published Guidelines Steven A. Farmer, MD PhD, James N. Kirkpatrick, MD University of Pennsylvania, Philadelphia, PA · Paul A. Heidenreich, MD MS, Stanford University, Palo Alto, CA · Jeptha P. Curtis, MD, Yongfei Wang, MS Yale University, New Haven, CT · Peter W. Groeneveld, MD MS, University of Pennsylvania, Philadelphia, PA; on behalf of the National Cardiovascular Data Registry Background and Objectives • Ethnic / racial disparities in cardiac care may partially result from over-provision of care among white patients. • We hypothesized that white patients were more likely than black and Hispanic patients to receive cardiac resynchronization therapy with defibrillator (CRT-D) devices outside of ACC/AHA/HRS guidelines. * Data are presented as number (percent) unless otherwise indicated. Methods Abbreviations: CRT–D Cardiac resynchronization therapy-Defibrillator; CHF–Congestive heart failure; RBBB–Right bundle branch block; LBBB–Left bundle branch block; LAFB-Left Anterior Fasciclular Block; LAPB-Left Posterior Fascicular Block; IVCD-Intraventricular Conduction Delay; SBP – systolic blood pressure; ESRD-End Stage Renal Disease • Data from the ACC-National Cardiovascular Data Registry (ACC-NCDR) for implantable cardioverter defibrillators (ICDs) from January 2005-April 2007. • We identified white, black and Hispanic patients who received CRT-D and then fit a multivariable hierarchical logistic regression model with full ACC/AHA/HRS guideline concordance (QRS duration ≥ 0.12ms, LVEF ≤ 35%, and class III or IV CHF) as a binary outcome variable. • Independent variables included race/ethnicity, age, gender, cardiomyopathy etiology, duration of CHF, blood pressure, QRS morphology, prior revascularization, atrial fibrillation / flutter, cerebrovascular disease, hypertension, diabetes, renal failure, and pulmonary disease. Conclusions Study Participants • After multivariate adjustment, we observed greater guideline-concordant use of CRT-D among black and Hispanic patients than among white patients. • Our findings suggest that racial /ethnic differences in CRT-D may be partially due to over-provision of this technology among white patients. Results • Of 108,341 registry patients, 39,088 CRT-D recipients were identified, including 33,310 (85%) white, 3,963 (10%) black, and 1,815 (5%) Hispanic patients. • Among CRT-D recipients, 9,430 (24%) patients lacked 1 CRT-D criterion, 1,840 (5%) patients lacked 2 criteria, and 217 (1%) patients lacked all 3 criteria. Specifically, 2,271 (6%) had an LVEF > 35%, 6,758 (17%) had class I/II CHF, and 4,732 (12%) had a QRS duration < 0.12 s • In multivariate analyses, black (OR 1.13, 1.04-1.23; p=0.004) and Hispanic (OR 1.10, 0.97-1.24; p=0.13) patients were more likely to meet all 3 CRT-D eligibility criteria than white patients. Implications • Nearly 30% of patients receiving CRT-D failed to meet one or more published criteria, and white patients were overrepresented in this group. • Receipt of CRT-D outside of guidelines exposes patients to the risks of implantation with less potential benefit. • Our findings indicate a need for more circumspect use of this expensive technology.