Download
1 / 21
240 likes | 785 Views
Update on Indications for Cardiac Resynchronization Therapy. Maria Rosa Costanzo, M.D., F.A.C.C., F.A.H.A. Medical Director, Midwest Heart Specialists-Advocate Medical Group Heart Failure and Pulmonary Arterial Hypertension Programs

E N D
Update on Indications for Cardiac Resynchronization Therapy Maria Rosa Costanzo, M.D., F.A.C.C., F.A.H.A. Medical Director, Midwest Heart Specialists-Advocate Medical Group Heart Failure and Pulmonary Arterial Hypertension Programs Medical Director, Edward Hospital Center for Advanced Heart Failure Naperville, Illinois, U.S.A.
Class I CRT is indicated for pts. who have LVEF ≤ 35%, SR, LBBB with a QRS duration ≥ 150 ms, and NYHA class II, III, or ambulatory IV symptoms on GDMT. Level of Evidence: A for NYHA class III/IV (MIRACLE, COMPANION, CARE-HF); Level of Evidence: B for NYHA class II (MADIT-CRT) Comments Modified recommendation specifying CRT in pts with LBBB of ≥150 ms expanded to include those with NYHA class II symptoms 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities Tracy CM et al. JACC 2012:60:1297-1311
Class IIa CRT can be useful for pts. with LVEF ≤ 35%, Sr, LBBB with a QRS duration 120 to 149 ms, and NYHA class II, III, or ambulatory IV symptoms on GDMT. (Level of Evidence: B) CRT can be useful for pts who have LVEF ≤ 35%, SR, a non-LBBB pattern with a QRS duration ≥ 150 ms, and NYHA class III/ambulatory class IV symptoms on GDMT. (Level of Evidence: A) CRT can be useful in pts. with AF and LVEF ≤ 35% on GDMT (Level of Evidence: B) if a) the patient requires ventricular pacing or otherwise meets CRT criteria and b) AV nodal ablation or pharmacologic rate control will allow near 100% ventricular pacing with CRT. CRT can be useful for pts. on GDMT who have LVEF ≤ 35% and are undergoing new or replacement device placement with anticipated requirement for significant (>40%) ventricular pacing). (Level of Evidence: C) Comments New recommendation New recommendation Modified recommendation (wording changed to indicate benefit based on EF rather than NYHA class; level of evidence changed from C to B). Modified recommendation (wording changed to indicate benefit based on EF and need for pacing rather than NYHA class); class changed from IIb to IIa). 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities
Class IIb CRT may be considered for pts. who have LVEF ≤ 30%, ischemic HF etiology SR, LBBB with a QRS duration ≥ 150 ms, and NYHA class I symptoms on GDMT. (Level of Evidence: C) CRT may be considered for pts. who have LVEF ≤ 35%, SR, a non-LBBB pattern with QRS duration 120 to 149 ms, and NYHA class III/ambulatory class IV on GDMT). (Level of Evidence: B) CRT may be considered for pts. who have LVEF ≤ 35%, SR, a non-LBBB pattern with a QRS duration ≥ 150 ms, and NYHA class II symptoms on GDMT. (Level of Evidence: B) Comments New recommendation New recommendation New recommendations 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities Tracy CM et al. JACC 2012:60:1297-1311
Class III CRT is not recommended for pts. with NYHA class I or II symptoms and non-LBBB pattern with QRS duration < 150 ms. (Level of Evidence: B) CRT is not indicated for pts whose comorbidities and/or frailty limit survival with good functional capacity to less than 1 year ). (Level of Evidence: C) Comments New recommendation Modified recommendation (wording changed to include cardiac as well as noncardiac comorbidities). 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities Tracy CM et al. JACC 2012:60:1297-1311
The Influence of Left Ventricular Ejection Fraction on the Effectiveness of Cardiac Resynchronization Therapy: MADIT-CRT Kutyifa V et al. JACC. 2013;61:936-944
The Influence of Left Ventricular Ejection Fraction on the Effectiveness of Cardiac Resynchronization Therapy: MADIT-CRT Kutyifa V et al. JACC. 2013;61:936-944
The Influence of Left Ventricular Ejection Fraction on the Effectiveness of Cardiac Resynchronization Therapy: MADIT-CRT Kutyifa V et al. JACC. 2013;61:936-944
Device Therapy in Heart Failure: Has CRT Changed “the Sickest Benefit the Most” to “the Healthiest Benefit the Most?” JACC 2013;61(9):945-947
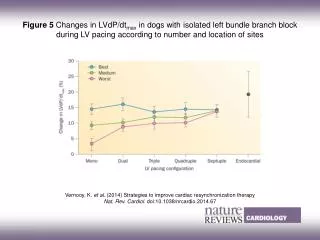
Differential Response to CRT by QRS Morphology and Duration Dupont M et al. JACC 2012; 60: 592-8
Histogram of QRS Duration in the Study Population Dupont M et al. JACC 2012; 60: 592-8
Echocardiographic and Clinical Response to CRT by QRS Morphology and Duration • After CRT, patients with LBBB morphology and/or QRS duration ≥ 150 ms had statistically significantly greater improvement in: • EF • LVEDD • LVESD • MR grade change • % of super-responders • NYHA functional class Dupont M et al. JACC 2012; 60: 592-8
Survival after CRT Implantation Dupont M et al. JACC 2012; 60: 592-8
Cox Proportional Hazards Models for Death, Heart transplantation and LAVD Placement Dupont M et al. JACC 2012; 60: 592-8
Changes in Echocardiographic Parameters in Super-Responder, Responder and Hyporesponder Groups Hsu JC et al. J Am Coll Cardiol. 2012; 59(25):2366-2373
Multivariable Analysis of Predictors of LVEF Super-Response Hsu JC et al. J Am Coll Cardiol. 2012; 59(25):2366-2373
Kaplan-Meier Estimates of Cumulative Probability of Heart Failure or Death, Death Alone, and Death or ICD Therapy for VT or VF Stratified by Response Category Hsu JC et al. J Am Coll Cardiol. 2012; 59(25):2366-2373
Cox Proportional Regression Analysis of Predictors of Nonfatal HF Events or Death Hsu JC et al. J Am Coll Cardiol. 2012; 59(25):2366-2373
Conclusions Since the publications of the Miracle trial the indications for CRT have evolved Measures of mechanical dyssinchrony have been largely disappointing in predicting response to CRT QRS duration has endured as the single stronger predictor of CRT response The MADIT-CRT trial has extended the indications for CRT to patients with prolonged QRS and mild HF symptoms The ability to predict non-responders to CRT remains elusive The ADVANCED-CRT Registry will help to characterize non-responders to CRT and to refine selection criteria for CRT