Download
1 / 44
590 likes | 1.4k Views
Cardiac Resynchronization Therapy (CRT). Vineeta Ahooja MD FACC Advanced Imaging, Cardiovascular Medicine Heart Health Institute. Vineeta Ahooja MD FACC Wayne State University 2000-2006 Internal Medicine and Cardiovascular Medicine

E N D
Cardiac Resynchronization Therapy (CRT) Vineeta Ahooja MD FACC Advanced Imaging, Cardiovascular Medicine Heart Health Institute
Vineeta Ahooja MD FACC Wayne State University 2000-2006 Internal Medicine and Cardiovascular Medicine Board certified: Internal Medicine, Cardiology, Comprehensive Echocardiography, Nuclear Cardiology and Cardiac CT Prior appointments: WSU-DMC, Lapeer RH, Mclaren Flint, William Beaumont, Genesys Current practice : Advanced cardiac imaging and general cardiology
3D ECHOCARDIOGRAPHY Assessment of Volumes/EF: Chemotherapy Anatomy : Prior to surgery Synchronicity : Heart Failure
SYNCHRONICITY INDEX TIME TO REACH MINIMUM SYTOLIC VOLUME FOR EACH SEGMENT AS PERCENTAGE OF THE CARDIAC CYCLE ALLOWS COMPARISON OF PATIENTS WITH DIFFERENT HEART RATES SDI CAN BE EXPRESSED IN MSEC CAN COMPARE SPECIFIC SEGMENTS IN THE HEART WITH THIS TECHNOLOGY AT THE SAME TIME THE STANDARD DEVIATION OF THE TMSV FOR EACH SEGMENT IS THE SYSTOLIC DYSYCHONICITY INDEX
VALUES SDI >3SD ABOVE THE MEAN FOR NORMAL SUBJECTS 8.3% MPI >=.7 SPWMD > 80 MSEC EDV>130 ML QRS >120 MSEC SPWMD> 130 MSEC HAS BEEN SHOWN TO CORRELATE WITH REVERSE REMODELING
THE PROBLEM IN PATIENTS WITH MODERATE AND SEVERE LVD • MPI AND SPWMD IDENTIFIED 76% AND 72% CORRECTLY • QRS>120MSEC JUST 46% PATIENTS WITH SIGNIFICANT DYSCHRONY
THREE D ECHO AND CRT CAN IT MAKE A DIFFERENCE ?
WHY THINK ABOUT CRT • 500,000 THOUSAND NEW CASES HEART FAILURE DIAGNOSED PER YEAR IN THE USA ( 50000 IN CANADA) • 25% ONE YEAR MORTALITY IN RECENT SWEDISH STUDY FOR DIAGNOSIS OF CHF • RECENT STUDIES SHOW DESPITE OPTIMAL MEDICAL DRUG TREATMENT MORTALITY REMAINS > 25% AT THREE YEARS • HOSPITAL ADMISSIONS AND OFFICE VISITS ARE FREQUENT FOR CHF PATIENTS FOLLOWING DIAGNOSIS • 20% OF PATIENTS WITH HEART FAILURE HAVE CONDUCTION DISEASE AND QRS > 120 MSEC • ABNORMAL VENTRICULAR ACTIVATION AND CONTRACTION HAS BECOME A THERAPUETIC TARGET IN PATIENTS WITH SEVERE SYMPTOMS AND REDUCTIONS IN LV FUNCTION • SUCCESSFUL CRT MAY CONFER AN MORTALITY BENEFIT
CRT IMPROVES QUALITY OF LIFE AND FUNCTIONAL CAPACITY IN THE RESPONDERS CRT MAY CONFER MORTALITY BENEFIT ALONE IN CORRECTLY SELECTED PATIENT IS QRS > 120 MSEC BEST SELECTION CRITERION ? THIS IS THE CURRENT RECOMMENDATION FOR CRT COMPLEX ECHO STUDIES SUGGEST LVMD IS PRESENT IN PATIENTS WITH NORMAL QRS AND SEVERE LV DYSFUNCTION NEW PARAMETERS ARE NECESSARY TO ASSESS THE CHF PATIENT WITH SEVERE LV DYSFUNCTION AND SYMPTOMS MORE COMPLETELY THE METHODS MUST BE CLINICALLY EASY TO IMPLEMENT INTO DAILY PRACTICE 30% WITH LBBB AND QRS>120 FAIL TO RESPOND TO CRT NEED TO CORRECTLY IDENTIFY THE NON REPONDERS UP FRONT CRT BACKGROUND INFO
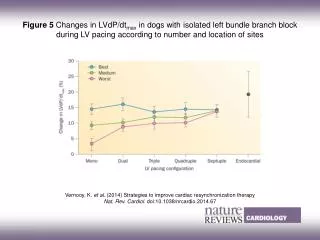
RT3DE AND CRT • ASSESS 16 SEGMENTS OF THE HEART FOR VOLUME • TIME TO MINIMUM SYSTOLIC VOLUME EASY TO SEE • USE THESE NUMBER TO PREDICT THE REPSONDERS • GET A 3D EF ALMOST EQUAL TO MRI ( R VALUE .9) • GET VOLUMES TO HELP MANAGE THE PATIENT • EDV GOOD PREDICTOR OF THE FUTURE ( SIMILAR TO MRI VALUE ) • MORE ACCURATE EF THAN 2D SIMPSON’S • SOME LABS NO LONGER DO 2DE EF
CONCLUSION • TMSV VARIATION <10% • CAN SEE DYSYCHRONY IN NORMAL AND VARIOUS GRADES OF LV DYSFUNCTION • MECHANICAL DYSSCHRONY IS PRESENT WITH INCREASING LV DYSFUNCTION BUT INDEPENDENT OF QRS DURATION • NO CORRELATION BETWEEN LVD AND PRESENCE OF SCARRED OR ANEURYSMAL SEGMENTS -IMPLYING LOCAL AREAS OF SCAR DO NOT CASUE DYSSYCHRONY PER SE BUT THIS IS DEPENDENT ON OVERALL LV SYSTOLIC FUNCTION • LOW EF < 20% AND SDI >15% MAY PREDICT RESPONSE BEST • RESPONDERS SAW DECREASE IN EDV AND INCREASE IN EF • SDI AND NORMAL OR SLIGHTLY REDUCED EF – IS CRT HELPFUL ? STUDY REMAINS TO BE DONE
TIME IT PEAK SYSTOLIC VELOCITY MEASURED ONSET QRS TO ORIGIN OR PEAK OF S2 WAVE DYSSYNCHRONY IF MAX DIFFERENCE BETWEEN TWO REGIONS BASAL AND LATERAL WALL SD OF 12 SEGMENTS ( BASAL AND MID SEGMENTS ) IN BOTH WALLS IN EACH OF THREE APICAL VIEWS TDI
REGIONAL TIME VOLUME CURVE APEX TO MITRAL VALVE ANNULUS WITH I SLICE
Indications for CRT are simple • NYHA III-IV on OPT • EF <35% LVEDD >55mm • SINUS RHYTHM • QRS >120ms • CLASS IA: ESC/AHA
Indications for CRT are simple • NYHA III-IV on OPT • EF <35% LVEDD >55mm • SINUS RHYTHM • QRS >120ms • CLASS IA: ESC/AHA What about those who don’t meet these criteria?