Download
1 / 15
150 likes | 258 Views
Distribute Project. Taha A. Kass-Hout, MD, MS Deputy Director for Information Science (Acting). Update to 2010 State Influenza Coordinator’s Conference Session Two – New and Enhanced Surveillance Sunday June 6, 2010 - 3:00-3:15pm, Portland, OR.

E N D
Distribute Project Taha A. Kass-Hout, MD, MS Deputy Director for Information Science (Acting) Update to 2010 State Influenza Coordinator’s ConferenceSession Two – New and Enhanced Surveillance Sunday June 6, 2010 - 3:00-3:15pm, Portland, OR Division of Healthcare Information (DHI) (proposed) Public Health Surveillance Program Office (proposed) Office of Surveillance, Epidemiology, & Laboratory Services (OSELS) (Proposed) Centers for Disease Control & Prevention (CDC) Disclaimer: The findings and conclusions in this presentation are those of the authors and do not necessarily represent the official position of The Centers for Disease Control and Prevention.
Principles & Characteristics • Aggregates counts of ILI and total ED visits from existing health dept ED-SS systems • Cross-tabulated by a limited number of variables • Allows flexibility in use of “chief complaint” (or ICD9) ILI Syndromic criteria that HDs had already developed • Fosters “community of users”
A Brief History of Distribute • Proof-of-concept Phase (2006 to July 2009) • Funding from CDC and Markle Foundation • Recruited nine sites in US and three internationally • Focused on establishing viability of approach • Pandemic Phase (August 2009 to June 2010) • Expanded funding from CDC lead to CDC, PHII and ISDS collaboration • Expanded from 10 to 34 sites (including 10 BioSense sites) in ~4months • Enhanced information systems, analyses • Strengthened community support
Current Status • ED Coverage Estimates • 34 Health departments (~1,300 EDs) with 8 HDs ≥ 90% ED visit coverage • Local ILI Syndrome Definitions • Narrow: attempts to replicate ILINet definition, may exclude many with influenza due to brevity of CC recording • Broad: less restrictive, yields parallel, higher amplitude signal
Information Pathways Via CDC Hospitals Hospitals HD SS system HD SS system Via ISDS (UW) Hospitals Hospitals HD SS system HD SS system Hospitals HD SS system CDC BioSense* Hospitals Hospitals CDC BioSense* * With HD approval
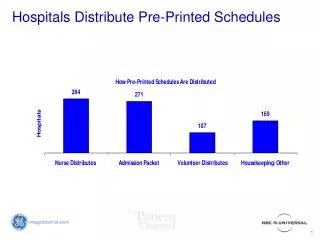
Stratifying Variables Number of Jurisdictions
Disposition (Admission) of ILI Pts Yellow: ILI patients hospitalized ILI patients Red: ILI patients hospitalized Total ED patients Green: ILI patients non-hospitalized Total ED patients % of ILI patients hospitalized % of ED visits by ILI patients not hospitalized % of ED visits by ILI patients who were hospitalized Week Ending Source: BioSense
Online Data Public Site http://ISDSDistribute.org Restricted(Contributor’s) Site
Comparison to ILINet • State-based jurisdictions • Correlations ranged from 0.64 to 0.96 with mean and median of 0.83 and 0.83, respectively • Local-based jurisdictions • Correlations ranged from 0.38 to 0.91 with mean and median of 0.76 and 0.81, respectively • Visually, major peaks in % ILI in the 2 systems tracked well together
Community of Practice • Approximately 90 state and local epidemiologists • Representing 43 health departments • Wide range of expertise in syndromic surveillance
Trade-Offs • Timeliness • Possible to collect and display daily, HD-specific ILI data (2-3 day lag for most HDs, including censoring for dates with incomplete reporting) • Instability of daily data: most recent 2-3 day “trends” not consistently born out by subsequent observations • Flexibility in ILI syndrome criteria • Allowed by using criteria “validated” by state/local flu surveillance experience • Variability in amplitude of signal precluded comparisons of H1N1 impact or summary estimate of H1N1 ED visits
Next Steps • Identification of EDs participating in Distribute and ILINet to prevent duplication • Assignment of ED surveillance POC at health departments and collaboration with influenza coordinators • ILINet and Distribute comparison • CSTE recommended continuing to display Distribute data separate from ILI-Net (aka, co-visualize) • Increase coverage (ongoing) • Address variability in ILI criteria (aka “Harmonize” ILI criteria)
Acknowledgements • ISDS Staff and Volunteers • Public Health Informatics Institute (PHII) • Project liaisons from NACCHO/CSTE/ASTHO • Support to ISDS • Tufts Health Care Institute (THCI) • Markle Foundation • CDC: • NCIRD, Influenza Division • OSELS & former NCPHI • H1N1 response team • OPHPR