Download
1 / 60
680 likes | 1.19k Views
Oxygen Transport and Asphyxia. AnS 536 Spring 2014. Goals. To transport oxygen from maternal blood across the placenta to fetal blood, and after birth from the lungs to the blood stream To move oxygen from blood to tissues to allow aerobic metabolism (efficient production of ATP)

E N D
Oxygen Transport and Asphyxia AnS 536 Spring 2014
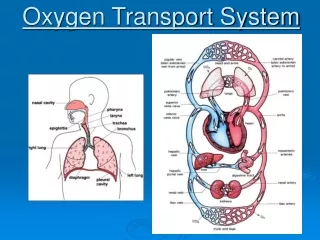
Goals To transport oxygen from maternal blood across the placenta to fetal blood, and after birth from the lungs to the blood stream To move oxygen from blood to tissues to allow aerobic metabolism (efficient production of ATP) To move carbon dioxide in the reverse direction
Erythrocytes • After maturation from stem cells in bone marrow, erythrocytes have a circulating life of ~120d • Highly specialized cells: • Cytoplasm contains ~35% solution of hemoglobin, but is devoid of subcellular organelles • Cannot synthesize nucleic acids or proteins, limited lipid metabolism • Carbohydrate metabolism devoted to maintaining functional pumps on cell membrane
Erythrocytes • After cell death, hemoglobin degraded and iron recycled to bone marrow • As they pass through capillaries, cells deform into ellipsoidal, hemispheric, or teardrop shapes • Cell fragility increased during newborn period • Increased risk and incidence of hemolytic diseases
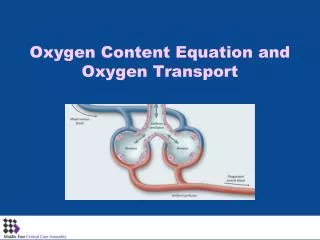
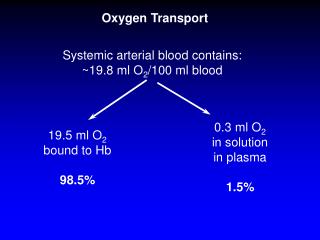
Transport of Gases in Blood • PO2 not only determines the dissolved oxygen content of blood, but also affects the amount of oxygen in reversible chemical combination with hemoglobin • Chemical and physiological actions of gases depend on the partial pressures they exert in the gas phase and in solution in various body fluids
Hemoglobin • The sigmoidal shape of the oxygen dissociation curve is physiologically important • Permits blood to deliver much more oxygen to tissues than a hyperbolic curve • The binding of one molecule of O2increases the affinity of the other sites for oxygen • Carbon dioxide binds to the globulin portions of the molecule rather than to the iron molecules • Accounts for about 10% of CO2 transport
Video Break http://www.dnatube.com/video/274/Hemoglobin-Oxygen-Binding http://www.youtube.com/watch?feature=player_detailpage&v=WXOBJEXxNEo
O2-Hb Dissociation Curve Illustrates a relationship between the partial pressure of oxygen (PO2) and percent saturated hemoglobin (Hb)
Hemoglobin • When Hb binds to oxygen, it undergoes a conformational change that releases H ions from globin chains, decreasing pH • Increasing pH in RBC will increase the affinity of Hb for oxygen • In capillaries H+ generated by carbonic anhydrase activity facilitates oxygen delivery to tissues (high CO2 concentrations)
Bohr and Haldane Effects • Bohr Effect • Describes the influence of CO2 and pH on the release of O2 • ↓ in pH (↑ in acidity) due to CO2 and hydrogen ions can combine reversibly with Hb at the sites other than the O2 binding sites (allosteric binding) • Results in a structural change of Hb, reducing its affinity for O2 • Haldane Effect • Displacement of O2 from Hb increases affinity for CO2 and hydrogen ions
Bohr and Haldane Effects • Work together facilitating O2 liberation and the uptake of CO2 and hydrogen ions at the tissue level • A Bohr or Haldane shift reduces Hb affinity for O2 • Important in placental O2 transport • pH is highest in arteries where O2 is picked up (umbilical and placental arterioles) • pH is lowest at venules after CO2 and hydrogen ions have been picked up • Changes in pH and CO2 on both maternal and fetal side of placenta regulate the rate of O2 transfer to a great extent
Bohr and Haldane Effects • Fetal pH is lower (more acidic) than maternal pH • Fetal acidosis is metabolic and not related to the high PCO2 • Primarily due to placentally produced lactate and pyruvate • The effect of low pH on O2 delivery to tissues is often overlooked, but may be important in maintaining O2 delivery to tissues at an appropriate rate
2,3-Bisphosphoglycerate(2,3-BPG) • Binds with greater affinity to deoxyhemoglobin • Once it binds to first binding site, it allosterically affects other sites in hemoglobin to effectively increase the rate of release of oxygen at tissue level • Right-shift of curve
HbF has a higher affinity for O2 than HbA Two alpha-gamma dimers rather than two alpha-beta dimers Creates a LEFT shift in the dissociation curve much like the effect of ↑ pH, ↓ temperature, or ↓ 2,3 BPG ↑ affinity for O2 by Hb in the fetal blood enhances O2 transport across the placenta After birth HbF declines as neonates begin to manufacture new erythrocytes and HbA HbF binds 2,3-BPG poorly Fetal Hemoglobin (HbF)
Cytochrome P450 • O2 is MUCH more soluble in lipids (like membranes) than in water (as in plasma or cytoplasm) • Cytochrome P450 enhances transport processes due to its high affinity for O2 and accumulates along the endoplasmic reticulum (ER) of placental cells • Many different varieties • Most involve drug metabolism • All incorporate oxygen into metabolic processes • Tissues can up- or down-regulate the levels of this molecule to enhance O2 transport into cell
Cytochrome P450 • ER forms channels from the cell membrane to the mitochondria allowing O2 to move more freely throughout or across the cell • Alignment of P450 along the ER channels creates a high affinity, O2 soluble freeway for O2 to travel • P450 enhances transplacental O2 transport • Studies have shown blocking P450 will decrease transplacental O2 flux by over 75%
Fetal Gas Exchange • CO2 diffuses across placenta primarily in molecular form - not as bicarbonate ion • Fetal PCO2 is higher than maternal • Fetal oxygen consumption is equivalent to adult values • Placenta is designed to protect the fetus from inadequate or excessive oxygen availability
Fetal Gas Exchange Cont… • Fetal mechanisms for protection against oxygen radicals are poorly developed prior to birth • Increased oxygen in fetal blood may have more adverse effects than beneficial effects • Induction of superoxide dismutase is due to increased exposure to oxygen postnatally
After Birth - O2 Binding to Hb • Factors affecting O2 binding to Hb in the lung • Primary factors • Perfusion of the area of the lung by blood • Ventilation rate of the newborn • Efficiency of exchange across the tissue • Other factors • Presence of fluid in the lung (if not cleared after first breath) • Presence of surfactant helps ventilation
After Birth - O2 Binding to Hb • Factors affecting O2 unloading at the tissues • Primary • Bohr and Haldane effects • Other factors • Failure to thermoregulate or low body temperatures • Shifts the Hb dissociation curve adversely to the LEFT • Higher affinity for O2, which is less likely to release oxygen to the tissue
Oxygen Transport from the Hemoglobin to the Mitochondria • Oxygen transport from the red blood cell (RBC) to the tissues occurs in the capillaries • RBC is deformed to an extent that the membrane is in direct contact with the cell membranes of the capillaries where O2 unloading occurs • O2 can move across a concentration and pressure gradient (high in the RBC) to the tissues (low gradient) • O2 then follows membranous channels created by the ER to move through the cells of the tissue being perfused
Oxygen Diffusion into Cells • Primary determinant of oxygen flow rate into a cell is the PO2 in the capillaries • Second determinant is rate that the cell consumes oxygen • Function of mitochondrial density
Oxygen Diffusion Cont… • Uneven spatial distribution of mitochondria within & between cells may allow both enhanced & parallel oxygen distribution & diffusion • Presence of myoglobin and/or cytochrome P450 permit diffusion facilitation in some tissues (brain, liver, placenta) • Cytochrome P450 aligns along endoplasmic reticulum as a high-affinity “bucket brigade” for oxygen - the ER forms a membranous channel (oxygen has higher solubility in fat than watery cytoplasm) from the cell membrane to the mitochondria • As PO2 decreases, extent of facilitation increases (increased ER channels, mitochondria move closer to outer sell membrane, and cytochrome P450 concentrations increase)
Newest Generation of Blood Substitutes or Hb Substitutes • Perfluorocarbon-based solutions • Offer very high affinity for oxygen • Carried in a solution rather than bound to Hb • O2 diffuses from an area of high concentration to low concentration whenever blood vessels are in close apposition to tissue • Useful when: • Blood volume has been compromised (as well as red blood cell count and Hb concentration) • Lung function is compromised (respiratory distress syndrome in infants)
Fetal PO2 22-29 mm Hg Hypoxic fetus per se Not true hypoxia as this value represents a normal range for this stage of life ↑ fetal O2 to adult values would be detrimental Fetal O2 consumption 3-4 mL/kg Equivalent to adult values ↑ affinity of HbF allows for greater saturation at any given partial pressure Fetal high cardiac output Most important compensatory mechanism O2 tensions ↓ tension may have teleological purpose Closure of the ductusarteriosus initiates at O2 tensions greater than 55 mm Hg O2 saturation in the fetus drops towards term Fetal, Newborn and Adult Hemoglobin Concentrations
Fetal, Newborn and Adult Hemoglobin Concentrations • O2 consumption is extremely high in newborns • Piglets • Starts at 9 mL/kg at 37º C • Raises to 25-30 mL/kg at 37º C • 3-fold increase over fetal levels (and adult levels) • Roughly corresponds to greater surface area/kg of the newborn relative to the adult • This ↑ in O2 consumption is necessary to maintain body temperature
Normal adult [Hb] 14-15 g/dL Newborn [Hb] 16-17 g/dL Fetal [Hb] vary [Hb] ↓ for the first few months after birth Blood volume ↑ Hematopoeisis is slow ↓ O2 carrying capacity at any given O2 tension Cattle Newborn Hb levels are much lower than in mature animals Roughly ½ that of adult levels Fragility of RBCs is increased during newborn period ↑ incidence of hemolytic diseases O2 radicals stimulate: Lipid peroxidation Intracellular proteolysis Hemolysis in erythrocytes Fetal, Newborn and Adult Hemoglobin Concentrations
Cesarian deliveries (calves) Significantly ↓ O2 tension and pH (7.0 vs 7.2) Significantly ↑ CO2 tensions as compared to vaginal deliveries Dystocia (calves) ↓ bicarbonate (17 mmol/L vs. 26 mmol/L) Severe lactic acidosis Slightly ↑ CO2 tensions Eutocic calves (1st 24 hrs) pH increases to ~7.4 CO2 remains steady O2 tension ↑ slowly to 70 mm Hg Bicarbonate ↑ slowly to 28 mmol/L Fetal, Newborn and Adult Hemoglobin Concentrations
Fetal Protective Mechanisms • Placenta is a protective barrier from inadequate and excessive oxygen availability • Either maternal hypoxia or hyperoxia will only have minimal effects on fetal oxygen concentrations • Fetal mechanisms for protection against oxygen radicals are poorly developed prior to birth • Increased O2 in the fetal blood may have more adverse effects than beneficial • Change of O2 at birth induces activity of several kidney and liver enzyme systems • Stability of O2 levels in the fetal system are critical to maintaining metabolic stability of the fetus
Oxygen Deficiency • Oxygen lack can be induced at any point in oxygen delivery system: • Reduced oxygen in ambient gas mixture that is inhaled • Impaired pulmonary exchange • Reduced oxygen content in blood • Impaired exchange at cellular level
Oxygen Deficiency Cont… • Chronic decreases in oxygen availability results in longer-term adaptive responses in delivery system • [Hb] increases (kidney medulla produces erythropoietin) • Affinity of Hb for oxygen may increase • Increase in rate and depth of ventilation • Increased cardiac output
Depends on acuteness or chronicity of condition Can potentially have long term detrimental effects Neurological and/or metabolic responses Hypoxic hypoxia Hyperventilation and ↓ metabolic response Tissue or organ damage Hypercapnic hypoxia ↓ in neural autoregulation Lack of response of neonate SIDS seen especially in newborns of smokers CO binds tightly to Hb, O2 not adequately exchanged Fetal Response to Hypoxia
Fetal Response to Hypoxia • Ischemic hypoxia • Severe neurodevelopmental disabilities • Can lead to death • Lactic acidosis due to anaerobic glycolysis • Cardiovascular function depressed • Intermittent hypoxia • Affect autonomic responses • Impaired performance in cognitive tasks
Neonatal Resistance to Hypoxia • First reference to neonates ability to withstand anoxia by Boyle (1670) • Kittens survived without oxygen longer then mature animals of same body weight • Earliest studies (Herman Kabat - late 1930’s) • Demonstrated that young animals could tolerate extended periods of complete stoppage of brain circulation to a greater extent than adults • The return of normal function was much faster in the neonate, even if the period of anoxia was longer • Survival time varies with maturity at birth • Newborn rats will survive 50 minutes in pure nitrogen compared to newborn guinea pigs that survive only 7 minutes • Guinea pigs are comparatively mature animals at birth
Neonatal Resistance to Hypoxia • Changes in heart function • Infant rats survived in nitrogen lived 50 minutes while the adults stopped breathing at 2-4 minutes • The heart continued to beat after cessation of breathing • Electrocardial alterations were noted
Neonatal Resistance to Hypoxia • Changes in regional blood flow • Altered in sheep during anoxia • O2 is conserved in crucial tissues at expense of hind limbs • Fetal animals • Preferential flow to the heart, brain, and adrenal glands • Limited placental and pulmonary flow • Loss of respiratory reflexes prior to loss of heart function • Brain flow maintains function in the midbrain, brainstem, and cerebellum at the expense of the cerebral cortex • Blood flow may decrease to other non-essential regions of the body to the point of permanent impairment after reperfusion • i.e. neonatal necrotizing enterocolitis
Neonatal Resistance to Hypoxia • Changes in energy status • Ability of neonate to obtain energy in the absence of O2 is critical for survival • 1931 – Reiss observed that whole body lactate content of asphyxiated neonates was 460% higher than baseline • 23% increase in asphyxiated adults • Large carbohydrate reserve was still available in neonate • Hypoglycemia reduces survival time by 50% in neonates
Neonatal Survival at Birth • Survival time also varies with maturity at birth • In term fetus, constriction of umbilical veins produce immediate bradycardia and decrease in arterial blood pressure • Constricting arterial flow or severing the cord will induce bradycardia with an increase in arterial pressure and increases carotid blood flow
Changes in Heart Function • Prior to delivery ~50% of fetal cardiac output directed towards the placenta • In bovine fetuses shortly prior to parturition subjected to anoxia by clamping umbilical cord, survival time was only 4 minutes • Heart activity continued for prolonged period after cessation of respiratory attempts
Free Radicals & Reactive Oxygen Metabolites • Oxygen can be toxic • Pure oxygen in ambient air is fatal to all mammals • Chronic exposure to high oxygen can destroy ability of carotid bodies to detect low oxygen concentrations • Most oxygen toxicity attributed to increased free radical production
Free Radicals • Reactive oxygen metabolites (ROM) generated as byproduct of cellular respiration and during respiratory burst responses of neutrophils and macrophages. • ROM reportedly contributes to aging, promotion of cancer, & initiation of inflammation. • Oxidative damage is non-specific for targets • Affects lipids, proteins, nucleic acids, carbohydrates, vitamins, and minerals
Nature of ROM • Various forms of ROM • Examples include superoxide anion, hydrogen peroxide, and hydroxyl radicals • All produced by sequential addition of a single electron to oxygen • Other free radicals formed that are physiologically important in neonatal period: • Ex: nitric oxide: acts as endothelium-derived relaxation factor for blood vessels
Nature of ROM Cont… • All free radicals have short half-lives • OH- half-life a nanosecond • O21 half-life 2 ms • NO half-life 4-6 s • By definition free radicals have unpaired electrons in outer orbital and are capable of independent existence • Oxidative potential of ROM due to configuration of outer electrons
Protective Mechanisms • ROM produced during normal metabolism of mammals • Protective mechanisms developed to scavenge radicals and minimize their damaging effects • Protective compounds included specific degradative enzymes, antioxidant vitamins, and others • Ex of vitamins: C, E, and carotenoids • Ex of enzymes: superoxide dismutase
ROMs in the Perinatal Period • Disorders associated with oxygenation of infants with respiratory distress syndrome include: chronic lung disease, retinopathy of prematurity, and intraventricular hemorrhage • Neonates have low circulating concentrations of vitamins E, C, and A at birth • Colostrum rich in fat-soluble vitamins and vitamin C, so high intake of colostrum important for premature infants or infants with respiratory distress.
Structural Features in Oxygen Delivery • Two factors to consider when looking at structure: • 1. Features which allow blood flow to be distributed to various organs and tissues in an appropriate amount • 2. Design properties which determine gas exchange between blood and the cells • Blood vessels permit oxygen delivery required by each tissue in proportion to the functional demands on the tissue