Download
1 / 39
390 likes | 412 Views
Dive into the body's regulating system closely linked to the nervous system, using glands and tissues to regulate growth, energy use, and more. Learn about hormones' role, secretion, and common disorders.

E N D
Endocrine System I’m hot, I’m cold, I’m fast, I’m slow. EMT-Paramedic Program
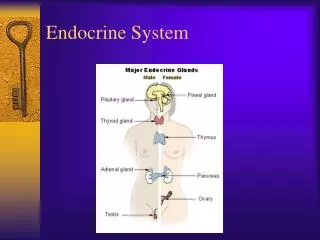
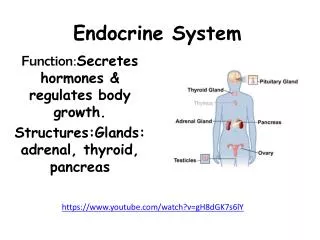
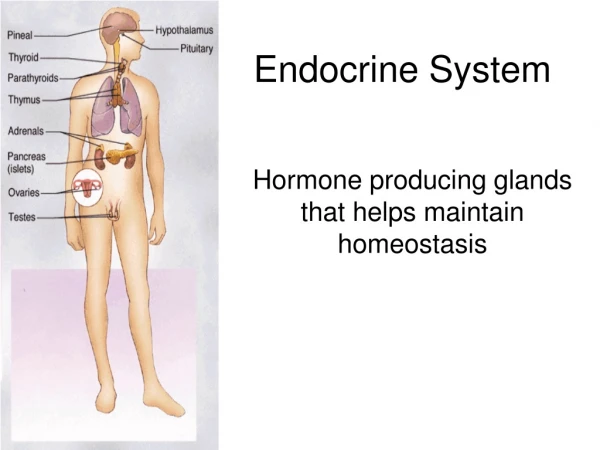
The System Itself • The other regulating system of the body • Closely linked to nervous system • Uses glands and tissues • Via hormones, the system regulates: • growth • the use of foods for energy • pH of body fluids • fluid balance • reproduction • provides resistance to stress
Chemical messengers to either: Body organs Tissues Or Both Binding depends on: Quantity Quality of receptor sites They may be divided into three groups: Amines Tyrosine, epi, norepi Proteins amino acids; insulin, GH, calcitonin, ADH, oxytocin Steroids cholesterol; cortisol, aldosterone, estrogen, progesterone, and testosterone Hormones
Hormone Secretion • Negative feedback mechanism • Endocrine glands respond to blood level changes or other hormones present • Secretion of hormone until stimulus is negated or changed
Pituitary “Master Gland” • Posterior holds hypothalamus hormones ADH and oxytocin • Anterior produces GH, TSH, ACTH, prolactin, FSH, LH
Specific Hormones • ADH • maintains BP by reabsorption of water by kidney tubules and vasoconstriction • Oxytocin • stimulates contraction of uterus and release of milk
Specific Hormones Thyroid Stimulating Hormone Growth Hormone Anterior Pituitary Adrenocorticotropic Hormone
Thyroid Gland • Produces: • T4 - Thyroxine • T3 – Triiodothyronine • Contain Iodine • Regulate energy production & growth • Calcitonin – • Regulates calcium • Maintains strong bones… • Also feeds back through pituitary
Parathyroid Glands • “Pair-a-thyroids?” • Produces parathyroid hormone • Also involved in calcium & blood phosphate levels
Disorders Associated with Thyroid Gland • Issues directly associated with gland • Tumor • Pituitary malfunction indirectly affecting • Hypothyroidism (Myxedema) • Hyperthyroidism (Grave’s Disease) • Thyrotoxicosis • Thyrotoxic Crisis (Thyroid Storm)
Disorders of the Thyroid Gland • Thyroid Storm • Severe Tachycardia, Dysrhythmias • Heart Failure • Shock • Hyperthermia • Restlessness, Agitation & Paranoia • Abdominal pain • Delirium, Coma • What else does this look like? • What could help you distinguish? • Danger in becoming a cynic?
Adrenal Glands Each adrenal has: • Medulla • -Epinephrine • -Norepinephrine • Cortex • -Aldosterone • -Cortisol
Trouble Associated with Adrenal Gland Cushing’s Syndrome • ACTH Levels too high • Enlarges adrenal gland • May be associated with pituitary tumor
Addison’s Disease Deficiency of cortisol & aldosterone Slow, gradual onset Progressive Fluid volume deficit Hyperpigmentation (bronze) Disorders Associated with Adrenal Glands
Adrenal Gland Disorders Addisonian Crisis • Acute episode preceded by: • Physical or emotional stress • Surgery • Alcohol intoxication • Trauma • Infection • Hypoglycemia • Adrenal cortex cannot comply with body’s increased demand
Ovaries Secrete • Estrogen • Progesterone progesterone
Testes Secrete • Testosterone • Inhibin
Pancreas • U R&L Q • Islets of Langerhans • Produce Glucagon & Insulin
Pancreatic Hormones • Glucagon – Alpha Cells • stimulates liver to change glycogen to glucose • raises blood glucose levels • Insulin – Beta Cells • lowers blood glucose levels by increasing transport of glucose into the cells
Glucose/Dextrose (D-glucose) • An intermediate in metabolism of carbohydrates • The most important carbohydrate, and is formed during digestion; absorbed from intestines into blood of portal vein; in passage through liver, is converted into glycogen
Glucose • May be: • Used immediately • Stored in muscles • Stored in fat • Brain cannot store it’s food • Requires continuous circulating volume • Reason neuro s/s develop quickly
Disorders Associated with Pancreatic Dysfunction Diabetes Mellitus • Hyperglycemia • Hypoglycemia • DKA • HHNK
Diabetes Mellitus • 16 million in North America. & rising • 3 diagnostic types: • IDDM Type I • NIDDM Type II • Other (Secondary) DM
Diabetes Mellitus • IDDM type 1 • Most commonly occurs in children and young adults • Genetic predisposition; Immune mediated destruction of insulin-producing cells
Diabetes Mellitus • NIDDM type II • Usually occurs after age 30. • A strong genetic predisposition is evident but pathogenesis is different. • Most individuals obese • Resistance to insulin action is present. • Exogenous insulin not required.
Promotion of Hyperglycemia • Increased dietary intake (esp. carbohydrates) • Limitation of physical activity • Reduction of hypoglycemic therapy • Limitation of endogenous insulin production • Pancreatic diseases • Drug treatment • Electrolyte disorders
Diabetes Mellitus • Other (secondary) DM • Associates hyperglycemia to another cause including: • Pancreatic disease/Pancreatectomy • Drugs or chemical agents • Others too • Gestational diabetes • Develops during pregnancy and resolves with birth but increased risk of DM later.
Development of Insulin Resistance • Infection • Inflammation • Myocardial ischemia or infarction • Trauma • Surgery • Emotional stress • Pregnancy • Drug treatment
S/S of Hyperglycemia/Insulin Insufficiency or Resistance • Polyuria • Polydipsia • Nocturia • Weight Loss • Fatigue • Blurred vision
Control • Oral • Transplant • Islet cells • Pancreas
Oral Hypoglycemic Drugs Metformin 500-1000 mg PO tid Avandia 4 mg PO qd
Diabetic Ketoacidosis • A result of severe insulin insufficiency and an excess of glucagon. Type I • Common causes: • Interruption of insulin therapy • Stress, infection • Non-compliance frequently a factor • Onset slow, from 12-24 hours.
Diabetic Ketoacidosis • Transition from glucose to lipid metabolism • Forms ketones & increase to toxic levels (diuresed) • Metabolic Acidosis • Symptoms • Causes severe osmotic diuresis and severe dehydration • Tx: Requires close monitoring • Draw red-top • Give IV fluids (Typically 3-5 L Low) • Consider thiamine • All vitamins & Electrolytes grossly deranged
Non-Ketotic Hyperglycemic Hyperosmolar Coma (HHNK) • Complication of Type II • Typically preceded by infection &/or diuretics • Hyperglycemic state causes hyperosmolar diuresis • Pronounced volume loss (Towards 10L) • CBG (PG) levels 1000 & higher • Only mild metabolic acidosis • Non-Ketotic • Many electrolytes within normal levels
Hypoglycemia • Common causes • Excessive insulin • Stress • Overexertion • Infection • Under eating • Symptoms • Treatment • O2, IV, CBG (Red Top), 50% dextrose IV
Endocrine Summary • A VERY complicated system • A specialty of it’s own • Much of EMS treatment is symptom oriented • Much of care is cause oriented • Important distinction