Download
1 / 28
290 likes | 469 Views
Gene Transfer for Neovascular Age-Related Macular Degeneration. Peter A. Campochiaro The Wilmer Eye Institute The Johns Hopkins University School of Medicine Baltimore, MD. Financial Disclosure. Research Support Genzyme Oxford BioMedica AskBio. Topics. Neovascular AMD Background

E N D
Gene Transfer for Neovascular Age-Related Macular Degeneration Peter A. Campochiaro The Wilmer Eye Institute The Johns Hopkins University School of Medicine Baltimore, MD
Financial Disclosure Research Support • Genzyme • Oxford BioMedica • AskBio
Topics Neovascular AMD Background Current Treatment Why Consider Gene Transfer? Endpoints for Clinical Trials Targeted Delivery Repeat Administration
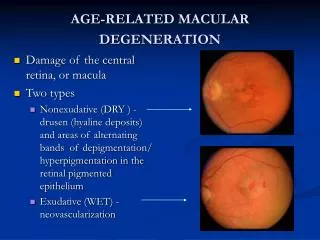
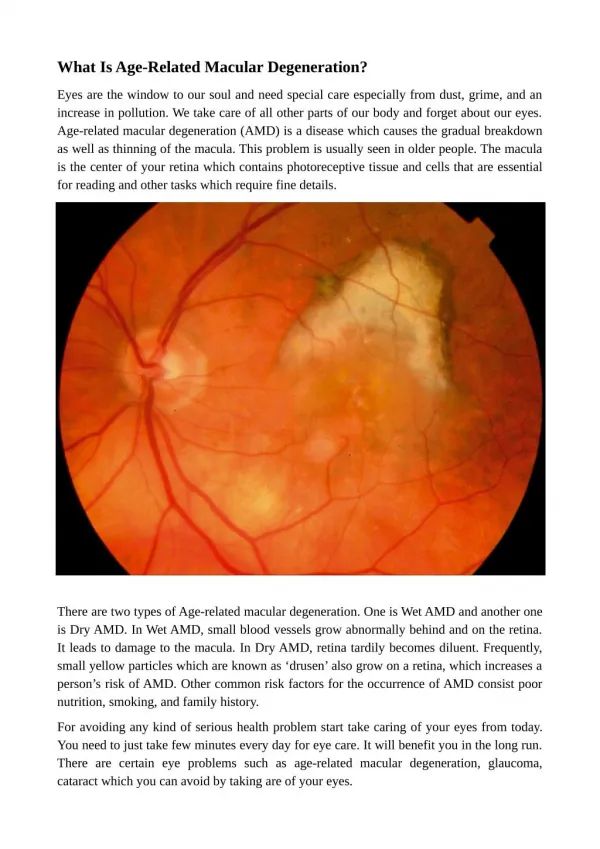
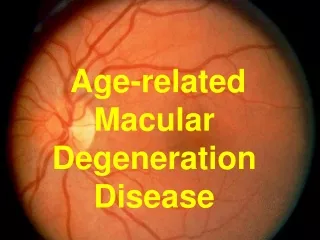
Age-Related Macular Degeneration (AMD) Early Intermediate Advanced Choroidal Neovascularization Geographic Atrophy Multiple small or a few intermediatedrusen Extensive intermediate drusen Subretinal Fibrosis
Advanced AMDMajor Public Health Problem Number of Individuals With Neovascular AMD or Geographic Atrophy (millions) No. of individuals (millions) 2000 2020
Ranibizumab for NVAMDMean Change in Visual Acuity Over Time * P < 0.0001 vs. sham 17.7 letter benefit * 17.0 letter benefit *
Subjects Gaining ≥15 Letters from BaselineMarina Trial % of patients 1-year outcomes 2-year outcomes Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 238) Sham (n = 240)
Why Consider Gene Transfer? Monthly intraocular injections provide best results Burden on patients and physicians Societal burden- expense Not feasible throughout most of the world Treatment as needed Increased risk of visual loss Gradual Catastrophic
AAV2.CBA-sFLT01 sFLT01– contains domain 2 of Flt-1 coupled by 9Gly linker to human IgG1 Fc - high affinity VEGF binding protein CBA promoter Packaged in rAAV2
Retinostat Endostatin and Angiostatin CMV promoter Packaged in Equine Infectious Anemia Viral (EIAV) Vector
Study Populations Subjects with AMD, aged 50 years or more with active CNV that shows evidence of active leaking on fluorescein angiography BCVA less than or equal to 20/200 in the study eye BCVA in the fellow eye of 20/200 or better Subjects unlikely to benefit from standard of care – subfoveal fibrosis 11
Endpoints • Primary Endpoint • The incidence of adverse events • Changes in best corrected visual acuity (BCVA) • Evidence of ocular inflammation • Intraocular pressure • Secondary Endpoints • The change from baseline in the amount of subretinal and intraretinal fluid measured by optical coherence tomography (OCT) • Change in size of active choroidal neovascularisation measured on fluorescein angiography • The change from baseline in BCVA at all time points • Transgene product levels in aqueous fluid 12
sFlt01 Trial • Two phases • Dose escalation • MTD evaluation • Dose escalation (Patients with limited visual potential due to macular scarring) • Four doses to be tested 2x108, 2x109, 6x109, 2x1010 vp • Minimum three patients per cohort • Patients enrolled to show safety and biological activity • MTD evaluation (Patients without scarring) • Two doses to be tested (MTD and one dose below) • Five patients per cohort • Patients enrolled to show safety, biological activity, possible efficacy
Retinostat Trial Cohort Dose level # of Patients Volume 1 1 3 300 µl 2 2 3 300 µl 3 3 3 300 µl 4 MTD 9 300 µl 14
Key information to be gained MTD Can vector cause reduction in amount of fluid within and under retina- measured by OCT? Level and duration of transgene product expression- measured in aqueous humor. Intravitreous vs subretinal injections
Advantages of Gene Transfer in NVAMD OCT provides a good quantitative outcome measure that allows us to assess biological activity even with poor visual potential We know what a good outcome should look like Secreted transgenes allow us to measure expression level over time- we should learn what levels are needed and if they are maintained long term.
Phase III Study Design and Endpoints VIEW 1 10.9 2q4 8.1 Rq4 7.9 2q8 6.9 0.5q4 Week
Phase III Study Design Visits q4wks- BCVA, eye exam, SD-OCT Primary Endpoint 52 weeks Group 1 Injection of vector dose 1 at baseline f/u visits- injection of RBZ if intraretinal or subretinal fluid Group 2 Injection of vector dose 2 at baseline f/u visits- injection of RBZ if intraretinal or subretinal fluid Group 3 Injection of RBZ at baseline f/u visits- injection of RBZ if intraretinal or subretinal fluid Group 4 Injection of RBZ at baseline f/u visits- injection of RBZ q visit
Phase III Endpoints Mean change in BCVA from baseline Number of injections of RBZ Need non-inferiority regarding BCVA Need superiority regarding # of injections of RBZ Secondary endpoints Intraretinal and subretinal fluid by OCT Size of active NV lesion by FA
Targeted Delivery Secreted transgene products so not necessary to deliver to diseased cell type However must target cells that are capable of robust and prolonged expression Vector, promoter, and route of injection are important
AAV2 Subretinal injection Transduction of retinal pigmented epithelium (RPE) and photoreceptors RPE-specific promoters can be used to exclude photoreceptors and other cells Very consistent among species including primates Intravitreous injection Ganglion cells, but differences among species
Lentiviral vectors Subretinal injection Transduction of retinal pigmented epithelium (RPE) and photoreceptors RPE-specific promoters can be used to exclude photoreceptors and other cells Very consistent among species including primates
Repeat Administration Long term expression after intraocular injection of AAV or lentiviral vectors in animals Determination of duration of expression in man is major objective of early phase trials
Fluocinolone Acetonide levels in the aqueous after single injection of sustained delivery pellet
Repeat Administration Treatment of fellow eye with gene transfer Since other treatments exist, not an urgent need Subretinal injection route has theoretical advantages
Gene Delivery for NVAMDConclusions Early phase trials will provide valuable information relevant to all ocular gene therapy Level and duration of expression with various vectors and routes of administration Quantitative endpoints (OCT) allow assessment of biological activity even in small trials and even when visual potential is limited Incorporating reduced injection burden into primary endpoint for phase III trials would be a major benefit