Download
1 / 17
230 likes | 1.38k Views
Radical Cystectomy As Early Primary Therapy for T1G3 Bladder Cancer. Karim Touijer and Bernard H. Bochner. Memorial Sloan-Kettering Cancer Center . T1G3 Bladder Cancer “THE FACTS”. Is a potentially lethal tumor This is NOT a superficial tumor Understaging occurs frequently

E N D
Radical Cystectomy As Early Primary Therapy for T1G3 Bladder Cancer Karim Touijer and Bernard H. Bochner. Memorial Sloan-Kettering Cancer Center
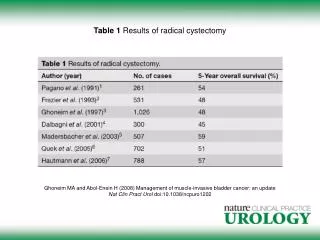
T1G3 Bladder Cancer“THE FACTS” • Is a potentially lethal tumor • This is NOT a superficial tumor • Understaging occurs frequently • High recurrence rate and progression despite intravesical therapy • Poor markers available to accurately identify high risk lesions • Can be effectively CURED by early definitive surgery (radical cystectomy)
9qDel Ta Ta RAS 9pDel (INK4A) NORMAL UROTHELIUM N+/M+ T1 T2-4 10qDel, 11pDel, 18qDel Tis TP53 RB 5qDel, 3pDel 14qDel N+/M+ T1 T2-4 (Presti et al, Ca Res 91; Cordon-Cardo et al, JNCI 92; Dalbagni et al, Lancet 93; Sarkis et al, JNCI 93; Cairns et al, Science 94; Orlow et al, JNCI 95; Li et al, Am J Path 96; Rabbani et al, JNCI 99; McShane et al, Ca Res 2000; Hernando et al, Int J Ca 2001; Sanchez et al, Ca Res, 2002; Veltman et al Ca Res, 2003 ) BLADDER CANCER:TWO PATHWAYS OF PROGRESSION
T1G3 Bladder CancerCan we accurately detect this disease?Are we at risk for understaging?
T1G3 And TIS Bladder CancerClinical Understaging 10 - 15% have positive nodes at cystectomy
Risk Of Understaging Is Influenced By Presence Of Muscle In TUR Specimen N=78 Dutta, J Urol 166:490, 2001 Herr, HW J Urol 162:74, 1999 A second TURBT required to identify extent of disease.
T1G3 Bladder CancerOutcome Of Understaged PatientsDisease Specific Outcomes • 179 patients (71% with T1 tumors) • 53% failed intravesical therapy • Understaged lesions do significantly worse • Understaged lesions WILL NOT respond to bladder sparing approaches Freeman et al, Cancer, 1995
Repeat TURBT May Help Reduce Understaging Dalbagni et al, UROLOGY 2002
T1G3 Bladder CancerNatural HistoryRecurrence and Progression Risk • Recurrence Risk • Following TURBT, 69-80% risk of recurrence • Intravesical immunotherapy can delay recurrence and progression, but long-term will not alter natural history • Progression Risk • 33-50% will progress to muscle invasion
BCG Can Delay Recurrence But May Not Impact Ultimate Cancer-specific Survival Recurrence-free survival Cancer-specific survival Orsola et al Eur Urol 48:231, 2005
T1G3 Bladder CancerLong-term Results With BCG Cookson, J Urol 158:62, 1997 Pansodoro, Urology 59:227, 2002 Shahin, J Urol 169:96, 2003
T1G3 Bladder CancerLong-Term Outcome ConservativeBCG and Progression of Disease • 1978-1981 86 patients with high risk non-muscle invasive disease (36 patients T1) • Randomized to TURBT +/- BCG • Followed q3-6 months for 3 years then annually • Evaluated progression and disease specific survival
T1G3 Bladder CancerLong-Term Outcome ConservativeBCG and Progression of Disease
T1G3 Bladder CancerLong-Term Outcome ConservativeDisease Specific Survival People not treated by cystectomy continue to die of bladder cancer! Cookson J Urol 158:62, 1997
T1G3 Bladder CancerLong-Term Outcome ConservativeDisease Specific Outcomes
T1 Bladder CancerCharacteristics Associated with Recurrence and Progression • Pathologic • High grade, multifocality, associated CIS, prostatic urethral involvement, size, sessile growth pattern, (Others unreliable and controversial: aneuplody, p53 alteration, lymphovascular invasion) • Clinical • Failure of intravesical therapy (80% with disease at 3 months progress), endoscopically uncontrollable disease, disease within diverticuli MAJORITY