Download
1 / 1
10 likes | 220 Views
No. 074. Indications and pathological outcomes of radical cystectomy. Stephanie Kerr, Prassannah Satasivam , Jeremy Grummet The Alfred Hospital, Prahran VIC. Introduction

E N D
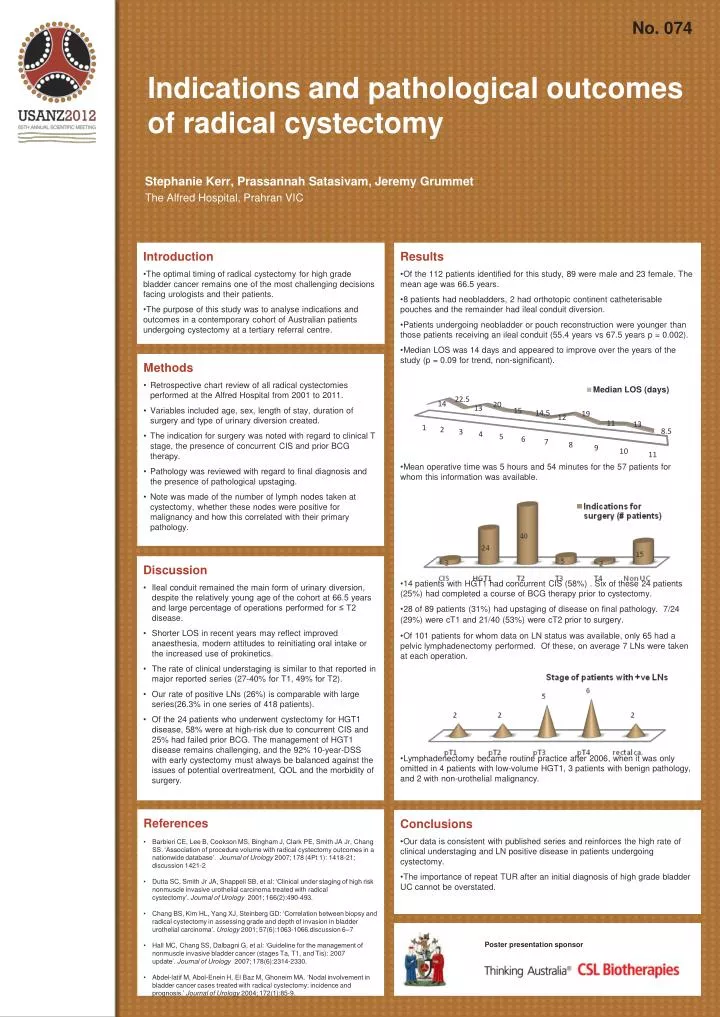
No. 074 Indications and pathological outcomes of radical cystectomy Stephanie Kerr, PrassannahSatasivam, Jeremy Grummet The Alfred Hospital, Prahran VIC • Introduction • The optimal timing of radical cystectomy for high grade bladder cancer remains one of the most challenging decisions facing urologists and their patients. • The purpose of this study was to analyse indications and outcomes in a contemporary cohort of Australian patients undergoing cystectomy at a tertiary referral centre. • Results • Of the 112 patients identified for this study, 89 were male and 23 female. The mean age was 66.5 years. • 8 patients had neobladders, 2 had orthotopic continent catheterisable pouches and the remainder had ileal conduit diversion. • Patients undergoing neobladder or pouch reconstruction were younger than those patients receiving an ileal conduit (55.4 years vs 67.5 years p = 0.002). • Median LOS was 14 days and appeared to improve over the years of the study (p = 0.09 for trend, non-significant). • Mean operative time was 5 hours and 54 minutes for the 57 patients for whom this information was available. • 14 patients with HGT1 had concurrent CIS (58%) . Six of these 24 patients (25%) had completed a course of BCG therapy prior to cystectomy. • 28 of 89 patients (31%) had upstaging of disease on final pathology. 7/24 (29%) were cT1 and 21/40 (53%) were cT2 prior to surgery. • Of 101 patients for whom data on LN status was available, only 65 had a pelvic lymphadenectomy performed. Of these, on average 7 LNs were taken at each operation. • Lymphadenectomy became routine practice after 2006, when it was only omitted in 4 patients with low-volume HGT1, 3 patients with benign pathology, and 2 with non-urothelial malignancy. • Methods • Retrospective chart review of all radical cystectomies performed at the Alfred Hospital from 2001 to 2011. • Variables included age, sex, length of stay, duration of surgery and type of urinary diversion created. • The indication for surgery was noted with regard to clinical T stage, the presence of concurrent CIS and prior BCG therapy. • Pathology was reviewed with regard to final diagnosis and the presence of pathological upstaging. • Note was made of the number of lymph nodes taken at cystectomy, whether these nodes were positive for malignancy and how this correlated with their primary pathology. • Discussion • Ileal conduit remained the main form of urinary diversion, despite the relatively young age of the cohort at 66.5 years and large percentage of operations performed for ≤ T2 disease. • Shorter LOS in recent years may reflect improved anaesthesia, modern attitudes to reinitiating oral intake or the increased use of prokinetics. • The rate of clinical understaging is similar to that reported in major reported series (27-40% for T1, 49% for T2). • Our rate of positive LNs (26%) is comparable with large series(26.3% in one series of 418 patients). • Of the 24 patients who underwent cystectomy for HGT1 disease, 58% were at high-risk due to concurrent CIS and 25% had failed prior BCG. The management of HGT1 disease remains challenging, and the 92% 10-year-DSS with early cystectomy must always be balanced against the issues of potential overtreatment, QOL and the morbidity of surgery. • References • Barbieri CE, Lee B, Cookson MS, Bingham J, Clark PE, Smith JA Jr, Chang SS. ‘Association of procedure volume with radical cystectomy outcomes in a nationwide database’. Journal of Urology 2007; 178 (4Pt 1): 1418-21; discussion 1421-2 • Dutta SC, Smith Jr JA, Shappell SB, et al: ‘Clinical under staging of high risk nonmuscle invasive urothelial carcinoma treated with radical cystectomy’. Journal of Urology 2001; 166(2):490-493. • Chang BS, Kim HL, Yang XJ, Steinberg GD: ‘Correlation between biopsy and radical cystectomy in assessing grade and depth of invasion in bladder urothelial carcinoma’. Urology 2001; 57(6):1063-1066.discussion 6–7 • Hall MC, Chang SS, Dalbagni G, et al: ‘Guideline for the management of nonmuscle invasive bladder cancer (stages Ta, T1, and Tis): 2007 update’. Journal of Urology 2007; 178(6):2314-2330. • Abdel-latif M, Abol-Enein H, El Baz M, Ghoneim MA. ‘Nodal involvement in bladder cancer cases treated with radical cystectomy: incidence and prognosis.’ Journal of Urology 2004; 172(1):85-9. • Conclusions • Our data is consistent with published series and reinforces the high rate of clinical understaging and LN positive disease in patients undergoing cystectomy. • The importance of repeat TUR after an initial diagnosis of high grade bladder UC cannot be overstated. Poster presentation sponsor