Download
1 / 32
320 likes | 527 Views
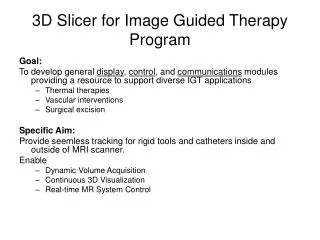
5-D Image Guided Cardiac Ablation Therapy. David R Holmes, III, Ph.D. Biomedical Imaging Resource. 4th NCIGT and NIH Image Guided Therapy Workshop October 13, 2011. Acknowledgments. Richard Robb, Ph.D. Douglas Packer, M.D. Maryam Rettmann, Ph.D. Fellows David Kwartowitz, Ph.D.

E N D
5-D Image Guided Cardiac Ablation Therapy David R Holmes, III, Ph.D. Biomedical Imaging Resource 4th NCIGT and NIH Image Guided Therapy Workshop October 13, 2011
Acknowledgments • Richard Robb, Ph.D. • Douglas Packer, M.D. • Maryam Rettmann, Ph.D. • Fellows • David Kwartowitz, Ph.D. • Jiquin Liu, Ph.D. • Cristian Linte, Ph.D. • Staff • Jon Camp • Bruce Cameron • Sue Johnson
Introduction • “If I can see it, I can fix it” • Thor Sundt to Rich Robb (1972) • Visualizing Cardiac Ablation • How can we best leveragethe available information tovisualize an ablation procedure? • Enhancing Visualization through Refinement • Visual Feedback of Ablation
Early Cardiac Ablation • Highly successful procedure (99%) • Some recurrence of fibrillation
Early Guidance for Cardiac Ablation • Real-time 3D feedback with functional information
Goal of high-dimensional/multi-modal imaging in RF cardiac ablation • Immerse the clinician in the patient • To see all of the data in the real-world context of the patient
Image Guided Cardiac Ablation Circa 1998 US Patent #6,556,695
Components of Multi-modal Image guidance • Registration • Needed for integration of signals • Context (Anatomy) • Needed to guide procedure • Parametric Mapping • Needed for presentation of data • Real-time Feedback • Needed to faithfully represent the patient on the table
Visualizing Cardiac Ablation Mapping Patient-Specific Anatomy
Image Guided Cardiac Ablation System Biosense System Single PC, Dual Display, Magnetic Field Generator, Catheter Panel Prototype System 4 Computational Servers, High Performance GUI, Dual Display with HUD, Digital Data Acquisition, Video Data Card, High-speed comm. network Phantom Exp. System Validation Phantom Dynamic Respirator Phantom Biosense Catheters Rettmann et al, 2006
Patient Procedures • To date, we have shadowed 4 procedures • Cardiologist uses CARTO XP for guidance • Mayo system captures all data • Cardiologist review after procedure
Ongoing Studies • Direct guidance with Mayo mapping system • Recording engineering metrics • Registration accuracy • Repeatability and targeting • Recording clinical metrics • Total procedure time • Time to burn • Patient success rates (eventually)
Enhancing Visualization through Refinement Fusing Intra-operative Data
Lessons Learned • Cardiologist “likes” the models, but doesn’t necessarily trust them • Image data anatomically faithful, but temporally inaccurate • The electro-anatomical map is temporally accurate, but low fidelity • ICE is temporally accurate and “high” resolution, but lacks the full 3D context • Data must be consistent to be trustworthy
Changing the way we look at the data • Stone Carving approach • Sampled points serve as the rough model • Enhance with high-resolution data • Paper Mache approach • Use the high-resolution pre-operative data as a scaffold for intra-operative data http://100swallows.wordpress.com/2009/05/20/how-to-carve-a-figure-in-marble/ http://www.flickr.com/photos/buildmakecraftbake/3239252403/
Updating Patient Models Current 3D Model Real-time Data Gross Registration (Tracking) Local Registration (Projection) Fuse Current Model with Local Features Liu et al, 2011
Synthetic experiment Liu et al, 2011
Patient Data (offline) Cameron et al, 2011
Ongoing Studies • Explore visualization techniques for fused models • Conduct targeting exercises with cardiologist to evaluate utility • In phantoms • In animal model
Visual Feedback of Ablation Modeling Thermal Response in LA
“Unsuccessful Ablation” • 30-50% patients have recurrence • Incomplete Isolation of PV • Temporary stunning masks true ablation • Inadequate visual feedback • Current ablation therapy guidance • Provide remedial representation of burn pattern • No information about the ablation • Temperature distribution, lesion size/pattern etc.
Approach • Enhance ablation therapy guidance by modeling thermal interaction using available data • High-resolution CT (pre-operative) as volumetric model • Intra-cardiac Echo (ICE) for local geometry • RF parameters from generator • Approximate tissue response to ablation using simplified thermal model
Thermal modeling of lesion growth with radiofrequency ablationdevicesIsaac A Chang*1 and Uyen D Nguyen2 BioMedical Engineering OnLine 2004, 3:27 doi:10.1186/1475-925X-3-27
Ongoing Studies • Ex-vivo studies underway to estimate tissue parameters and validate model • In-vivo animal studies in early 2012 • Retrospectively analyze clinical cases to determine predictability of the model
Concluding Remarks • “If I can see it ….” is necessary, but not sufficient. • “If I can see if and believe it…” • Thus, we put specific emphasis on: • what the clinician wants. • what we can learn from the data. • What we can validate