Download
1 / 20
200 likes | 572 Views
Cardiac Resynchronisation Therapy. September 2008. The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure (CARE-HF).

E N D
Cardiac Resynchronisation Therapy September 2008
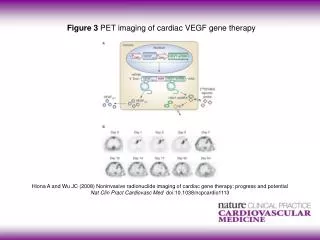
The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure (CARE-HF) John G.F. Cleland, M.D., Jean-Claude Daubert, M.D., Erland Erdmann, M.D., Nick Freemantle, Ph.D., Daniel Gras, M.D., Lukas Kappenberger, M.D. and Luigi Tavazzi, M.D. N Engl J Med Volume 352;15:1539-1549 April 14, 2005
Background • Despite pharmacological advances in treatment of HF, mortality & morbidity remain high • Cardiac dyssynchrony (regions of delayed myocardial activation & contraction) is common • Small studies (up to 6/12) cardiac resynchronisation therapy (CRT) improved quality of life, exercise capacity & ventricular function • Trials with CRT +/- ICD (COMPANION) showed that with CRT alone the decrease in risk of death was insignificant • Meta-analysis are inconclusive • This trial was designed to assess the effect of CRT on mortality in patients with severe HF
Methods • Multicenter, randomised, non blinded, international trial comparing “the risk of complications & death of standard pharmacological therapy alone with that of combination of standard therapy and CRT (without ICD) in patients with LV systolic dysfunction, cardiac dyssynchrony and symptomatic heart failure” • 82 European centers between Jan 2001 & March 2003 Inclusion Criteria: • 18yrs+ • HF for at least 6 weeks • NYHA III/IV • LVEF < 35% • QRS of at least 120ms Exclusion Criteria: • Conventional indications for PPM/ICD • Major CV event in last 6/52 • HF requiring IV therapy • Atrial arrhythymias
Methods • End Points • Primary: Composite of death from any cause or an unplanned hospitalisation for major CV event (worsening HF, MI, USA, Stroke, Arrhythmia) • Secondary: Death from any cause, Quality of life assessment • Statistical Analysis • Intention to treat Principle • Statistical power of 80% to identify a 14% relative reduction given an α value of 0.025 & predicted number of events as 300
Baseline Characteristics of the Patients Cleland, J. et al. N Engl J Med 2005;352:1539-1549
Kaplan-Meier Estimates of the Time to the Primary End Point (Panel A) and the Principal Secondary Outcome (Panel B) Cleland, J. et al. N Engl J Med 2005;352:1539-1549
Study Outcomes in Analyses Stratified According to NYHA Class Cleland, J. et al. N Engl J Med 2005;352:1539-1549
Hemodynamic, Echocardiographic, and Biochemical Assessments Cleland, J. et al. N Engl J Med 2005;352:1539-1549
Discussion • CRT substantially reduced risk of complications & death among patients with moderate/severe heart failure • Consistent with a reduction in cardiac dyssynchrony leading to improved physiological parameters and clinical outcome: • Quality of Life • Ventricular function • Blood pressure • Mortality • For every 9 devices implanted 1 death and 3 hospitalisations are prevented
Background1 • Approx 25% of patients with CHF have intraventricular conduction delay; commonly LBBB • Electrical activation of lateral aspect of LV can be delayed in relation to that of RV and/or interventricular septum • This results in • Dyssynchronous electrical activation & contraction • Unequal distribution of myocardial workload • Altered myocardial blood flow & metabolism • Patients with conducting disease have worse prognosis from CHF • Patients with a paced RV end up having an artificially induced interventricular conducting delay and overall systolic function is poorer
Procedure2 • Simultaneous pacing of RV & LV = Biventricular pacing • RA, RV & LV • LV paced via coronary sinus
Physiological Effects • Doesn’t restore normal physiological conducting pattern • RA pacing with short AV delay ensures all beats are paced • RV & LV pacing reduces the delay in electrical activation of LV free wall • QRS duration tends to decrease Haemodynamic response: • Increase in rate of rise of LV pressure • Increases pulse pressure, LV stroke volume • Improves myocardial function without increasing myocardial energy consumption
Evidence • Early Trials: <500 patients, up to 1 year showed increases in functional capacity & improvements in quality of life • COMPANION3(ICD): mortality from all causes was reduced with CRT & ICD (p=0.003) but not from CRT alone (p=0.059) • CARE-HF4: mortality from all causes was reduced (p<0.002)
Guidance for CRT5 NICE May 2007; must fulfil ALL the below • NYHA III or IV • SR with QRS >150ms • SR with QRS 120-149ms & echo evidence of dyssynchrony • LVEF < 35% • Optimal pharmacological therapy Cost: £3809 Number: 500/year
Guidance for CRT-D6 NICE May 2007 & January 2006 • Criteria as before plus: • Primary Prevention • MI (>4/52) & either (LVEF <35% and NSVT on holter and inducible VT on EP studies) OR (LVEF <30% and QRS >120ms) • Familial Tendency (longQT, Brugada, HOCM, ARVD) • Secondary Prevention (in absence of treatable cause) • Post VT/VF arrest • Spontaneous sustained VT causing compromise • Sustained VT without compromise but LVEF >35% Cost: £16000 Number: 500/year
Adverse Effects • Unable to implant LV lead due to unfavourable anatomy (3-10%) • Diaphragmatic stimulation due to proximity of phrenic nerve • Coronary sinus dissection (0.3-4.0%) • Coronary sinus perforation & tamponade (0.8-2.0%) • Periprocedural death (0.4%) • Dislodgement of LV lead (10%) • Pneumothorax • Complete Heart Block • Asystole • Pacemaker pocket infection • External electromagnetic field
Further Study • ? Benefit in NYHA I/II patients • REVERSE7: no significance at end point • MADIT-CRT: late 2009 • Approx. 20-30% of patients with CRT are non-responders • Is the QRS duration a good predictor of CRT response? • Could echo evidence of ventricular dyssynchrony be more predictive?8 • “Dyssynhcrony study”9 • Application in patients with AF?
References • Jarcho JA. Biventricular Pacing. N Engl J Med 2006;355:288-294 http://content.nejm.org/cgi/content/full/355/3/288 • Jarcho JA. Resynchronising Ventricular Contraction in Heart Failure. N Engl J Med 2005;352:1594-1597 http://content.nejm.org/cgi/content/full/352/15/1594 • Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. (COMPANION) N Engl J Med 2004;350:2140-2150 http://content.nejm.org/cgi/content/full/352/15/1539 • Cleland JGF, Daubert J-C, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure (CARE-HF) N Engl J Med 2005;352:1539-1549 http://content.nejm.org/cgi/content/full/350/21/2140 • NICE: Heart Failure – Cardiac Resynchronisation; May 2007 http://www.nice.org.uk/TA120 • NICE: Arrhythmias – Implantable Cardioverter defibrillators: January 2006 http://www.nice.org.uk/TA95 • Linde C, Abraham WT, Gold MR, Daubert J-C. Results of the REVERSE trial. Program and abstracts from the American College of Cardiology 2008 Scientific Sessions, March 29-April 1, 2008, Chicago, Illinois http://www.medscape.com/viewarticle/573311 • Yu CM, Bax JJ, Monaghan M, Nihoyannopoulos. Echocardiographic evaluation of cardiac dyssynchrony for predicting a favourable response to cardiac resynchronisation therapy. Heart 2004;90:vi17-vi22 http://heart.bmj.com/cgi/content/full/90/suppl_6/vi17 • Bax JJ, Ansalone G, Breithardt et al. Echocardiographic evaluation of CRT: ready for routine clinical use? J Am Coll Cardiol 2004;44:1-9 http://content.onlinejacc.org/cgi/content/full/44/1/1