Download
1 / 56
580 likes | 845 Views
The Arrhythmias . Ibrahim Sales, Pharm.D . Assistant Professor of Clinical Pharmacy King Saud University isales@ksu.edu.sa. Key Concepts. Use of antiarrhythmic drugs in the US has declined due to major trials showing increased mortality associated with use

E N D
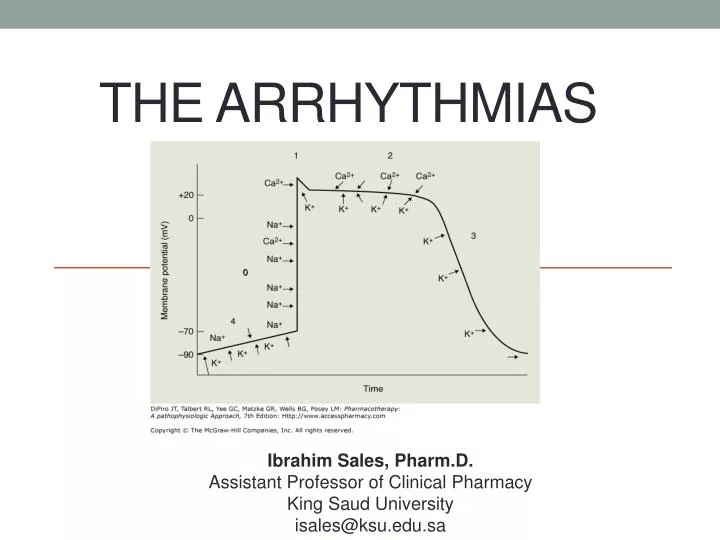
The Arrhythmias Ibrahim Sales, Pharm.D. Assistant Professor of Clinical Pharmacy King Saud University isales@ksu.edu.sa
Key Concepts • Use of antiarrhythmic drugs in the US has declined due to major trials showing increased mortality associated with use • recognition of proarrhythmia as significant adverse effect • advancements in nondrug therapy technology • ablation • implantable cardioverter-defibrillator (ICD) • Antiarrhythmic medications frequently cause adverse effects, complex pharmacokinetics
Normal Conduction • Electrical activity initiated at sinoatrial (SA) node • highest rate of spontaneous impulse generation • Moves through cardiac tissue to ventricles at the atrioventricular (AV) node • Flows down bundle of His to bundle branches & the Purkinje system • 2 bundle branches on left; 1 on the right • Impulse reaches refractory tissue (recently excited) & dies out • SA node recovers & fires again
Normal Conduction of the Heart • Inherent HR • SA node • 60-100 bpm • AV JUNCTION • 40-60bpm • VENTRICULAR • 20-40 bpm
Normal Conduction • Phase 0: initial, rapid depolarization of atrial & ventricular tissues; increase in cell Na+ permeability; Na+ influx; rapid depolarization overshoots electrical potential, brief period of repolarization • Phase 1: transient active K+ efflux; Ca2+ influx • Phase 2: Ca2+ influx balanced by K+ efflux; plateau • Phase 3: membrane permeable to K+ efflux; repolarization • Phase 4: gradual depolarization; constant Na+ leak to intracellular space balanced by K+ efflux
Abnormal Conduction • Tachyarrhythmia: 2 categories • abnormal impulse generation • “automatic” tachycardia • abnormal impulse conduction • “reentrant” tachycardia
Reentrant Tachycardias • Three conditions required: • two pathways for impulse conduction • an area of unidirectional block (prolonged refractoriness) in one of these pathways • slow conduction in the other pathway
Antiarrhythmic Drugs • Vaughan Williams classification limitations • incomplete, does not include digoxin, adenosine • many agents have properties of more than 1 class • does not incorporate mechanism of tachycardia termination/prevention, clinical indications, side effects • agents “labeled” within a class
Classification of Antiarrhythmic Drugs aVariables for normal tissue models in ventricular tissue. bAlso has type II, β-blocking actions. cClassification controversial. d Not clinically manifest. eVariables for SA & AV nodal tissue only. fAlso has sodium, calcium, β-blocking actions DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
AADs Have distinct Characteristics depending on which ion channels they block Ca+ Class IV: CCB Class IV Class I: quinidine, procainamide, dispopyramide, lidocaine Flecainide propafenone 0 mV Class III Class III: amiodarone, dofetilide, dronedarone, sotalol, ibulitide Na+ K+ Class I -90mV Class II: Beta Blockers Class II Ca+
Type I Agents • Block Na+ conduction: “plug up” channels • Channel state affinity • lidocaine, flecainide: block during inactivated state • quinidine: binds when channel is open/activated • Binding & unbinding specific to the receptor • Type Ia: intermediate binding kinetics • Type Ib: fast receptor binding/dissociation • Type Ic: slow receptor binding/dissociation
Type Ia Antiarrhythmics • Quinidine, procainamide, disopyramide • Slow conduction velocity, prolong refractoriness, decrease automatic properties of Na+ dependent conduction tissue • reentry: transform area of unidirectional block into bidirectional block • wave cannot get through pathway in retrograde fashion • area still refractory • Primarily Na+ channel blockers • some effects attributed to K+ channel blockade • used for supraventricular & ventricular arrhythmias
Type Ib Antiarrhythmics • Lidocaine, mexiletine: weak Na+ channel antagonists • Shorten refractoriness without affecting conduction velocity; improve antegrade conduction & eliminate unidirectional block • Used primarily in ventricular arrhythmias
Type Ib Antiarrhythmics • Lidocaine • Indicated for Pulseless VT/VF conversion or VT with a pulse. VT maintenance • PK: Reduce dose in those with HF, liver disease, low body weight and renal dysfunction and in the elderly • DI: Amiodarone (increased lidocaine levels) • Mexiletine • VT maintenance
Type IcAntiarrhythmics • Propafenone, flecainide • Profoundly slow conduction velocity • Refractoriness relatively unaltered • Eliminate reentry: slow conduction to point where impulse is extinguished & cannot propagate • Potent Na+ blockers • Effective for both ventricular & supraventricular arrhythmias • ventricular arrhythmia use limited by proarrhythmia risk
Type IcAntiarrhythmics • Propafenone, Flecainide • Indicated for patients with AF without structural heart disease. • Avoid in patients with LV dysfunction and/or CAD. • Can be initiated in an outpatient setting for patients with paroxysmal atrial fibrillation and no associated structural heart disease • Follow-up: • frequent ECG monitoring or via transtelephonic monitoring for potential signs of proarrhythmia.
Type II Agents • β-blockers • Antiarrythmic mechanism: anti-adrenergic actions • SA & AV nodes influenced by adrenergic innervation • Adrenergic stimulation increases conduction velocity, shortens refractoriness & increases automaticity of nodal tissues • β-blockers antagonize these effects • useful for exercise related tachycardias or other tachycardias induced by high sympathetic tone
Non-Acute Setting and Chronic Maintenance Rate Control Therapy of Atrial Fibrillation
Type III Agents • Amiodarone, sotalol, ibutilide, dofetilide • Prolong refractoriness in atrial & ventricular tissue • Delay repolarization: block K+ channels • Danger of blocking K+ channel too much: causes arrhythmias such as Torsades de Pointes (TdP)
Type III Agents • Amiodarone & sotalol: effective in most supraventicular & ventricular tachycardias • Sotalol inhibits outward K+ movement during repolarization; nonselective β-blocking actions • Hospitalization mandatory for initiation, • obtain QT 2–3 hours after first 5 doses, may increase dose after 3 days; NTE QT > 500 milliseconds • Not effective for AF conversion
Case 1 A 52-year-old man comes into the clinic with a medical history significant for atrial fibrillation, diabetes, and hypertension. Current medications include metoprolol tartrate 100 mg twice daily, glyburide 10 mg twice daily, lisinopril 40 mg/day, and hydrochlorothiazide 25 mg/day. He comes to the clinic today with shortness of breath and fatigue. An ECG shows that he is in atrial fibrillation. The physician would like to admit the patient and start dofetilide.
Case 1 Which one of the following medications should be discontinued before dofetilide is initiated? A. Glyburide.B. Metoprolol.C. Hydrochlorothiazide. D. Lisinopril.
Type III Agents • Dofetilide (oral only) & ibutilide (IV only) • used for acute conversion of AF or atrial flutter to sinus rhythm • block rapid component of the delayed K+ rectifier current • Dofetilidecan be used to maintain sinus rhythm after conversion • Ibutilide requires ECG monitoring during and 4 hours after infusion • DIs: CYP 3A4 inhibitors or drugs secreted by the kidney (ketoconazole, verapamil, trimethoprim, megestrol); HCTZ should be d/c’d as concentrations of dofetilide increase (hypokalemia, hypomagnesemia, increases the concentration of dofetilide inhibition of renal tubular secretion)
Case 1 A 52-year-old man comes into the clinic with a medical history significant for atrial fibrillation, diabetes, and hypertension. Current medications include metoprolol tartrate 100 mg twice daily, glyburide 10 mg twice daily, lisinopril 40 mg/day, and hydrochlorothiazide 25 mg/day. He comes to the clinic today with shortness of breath and fatigue. An ECG shows that he is in atrial fibrillation. The physician would like to admit the patient and start dofetilide.
Case 1 Which one of the following medications should be discontinued before dofetilide is initiated? A. Glyburide.B. Metoprolol.C. Hydrochlorothiazide. D. Lisinopril.
Case 2 For a 42-year-old man with atrial fibrillation who did not respond to class Ic agents, the electrophysiologist started dofetilide 500 mcg twice daily in the hospital 2 weeks ago. He comes to the clinic today for a follow-up. An ECG was done today showing normal sinus rhythm and QTc of 0.455 seconds (baseline QTc 0.395 seconds). The only medication change was the initiation of azithromycin yesterday for bacterial sinusitis.
Case 2 Because this drug was initiated, which one of the following changes needs to take place and why? • Discontinue azithromycin, administer an alternative antibiotic, and have patient return in 2 days for repeat ECG. • Finish course of azithromycin, decrease dose of dofetilide to 125 mcg twice daily, and have patient return in 3–7 days for repeat ECG. • Finish course of azithromycin, continue current dose of dofetilide at 500 mcg twice daily, and have patient return in 2 days for repeat ECG to reevaluate. • Withdraw dofetilide and return to clinic in 3–7 days for repeat ECG.
Dofetilide Dosing • AF conversion: • 500mcg PO twice daily (CrCl>60mL/min) • 250mcg PO twice daily (CrCl 40-60mL/min) • 125mcg PO twice daily (20-40mL/min) • Contraindicated CrCl<20mL/min • AF maintenance: Titrate down on the basis of QTc • Must be started inpatient. Determine QTc 2-3 hours after initial dose. If QTc increases by>15% or >0.5 sec, reduce dose by half. • Need a 3-month washout period if initiated after amiodarone failure
Case 2 For a 42-year-old man with atrial fibrillation who did not respond to class Ic agents, the electrophysiologist started dofetilide 500 mcg twice daily in the hospital 2 weeks ago. He comes to the clinic today for a follow-up. An ECG was done today showing normal sinus rhythm and QTc of 0.455 seconds (baseline QTc 0.395 seconds). The only medication change was the initiation of azithromycin yesterday for bacterial sinusitis.
Case 2 Because this drug was initiated, which one of the following changes needs to take place and why? • Discontinue azithromycin, administer an alternative antibiotic, and have patient return in 2 days for repeat ECG. • Finish course of azithromycin, decrease dose of dofetilide to 125 mcg twice daily, and have patient return in 3–7 days for repeat ECG. • Finish course of azithromycin, continue current dose of dofetilide at 500 mcg twice daily, and have patient return in 2 days for repeat ECG to reevaluate. • Withdraw dofetilide and return to clinic in 3–7 days for repeat ECG.
Case 3 A 65-year-old man was admitted to the hospital after several shocks from his implantable cardiac defibrillator (ICD) caused by episodes of ventricular tachycardia (VT). He was placed on amiodarone during his admission and was discharged on 400 mg/day. He presents to the clinic two weeks later for a follow-up. You evaluate his chart to make sure that baseline monitoring has been done. You find that he had a thyroid panel and chest radiograph performed while an inpatient.
Case 3 Which one of the following laboratory/baseline monitoring parameters also needs to be obtained because amiodarone is being initiated? A. LFTs.B. CBC.C. Lipid panel. D. Electrolytes.
Amiodarone • Characteristics of all Vaughan Williams classes • Na+ channel blocker with fast on/off kinetics • noncompetitive, nonselective β-blocker actions • blocks K+ channels • small degree of Ca2+ antagonist activity • Quick onset with IV administration • Initial action: β-blockade • Predominant effect with chronic use: prolongation of repolarization • Low proarrhythmic potential
Time Course & Electrophysiologic Effects of Amiodarone aRate-dependent. AERP, atrial effective refractory period; AH, atria-His interval; ECG, electrocardiographic effects; EP, electrophysiologic actions; HR, heart rate; HV, His-ventricle interval; VERP, ventricular effective refractory period. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Amiodarone • Most commonly prescribed antiarrhythmic • Used in chronic & acute supraventricular/ventricular arrhythmias • Unusual pharmacologic effects, pharmacokinetics, dosing, adverse effects • extremely long t½ (15 to 100 days) • large volume of distribution (Vd) • inhibits P-glycoprotein & most CYP-P450 enzymes • many drug interactions • severe multi-organ toxicities with chronic use
Amiodarone Dosing • AF conversion • IV: 5-7mg/kg IV over 30-60min.; then 1.2-1.8g/day; continue IV or divided doses until 10g total • PO (inpatient): 1.2-1.8g/day in divided doses until 10g total • PO (outpatient) 400mg/day x 2-4 weeks • AF maintenance • 100-400mg/day
Amiodarone Monitoring DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com
Case 3 A 65-year-old man was admitted to the hospital after several shocks from his implantable cardiac defibrillator (ICD) caused by episodes of ventricular tachycardia (VT). He was placed on amiodarone during his admission and was discharged on 400 mg/day. He presents to the clinic two weeks later for a follow-up. You evaluate his chart to make sure that baseline monitoring has been done. You find that he had a thyroid panel and chest radiograph performed while an inpatient.
Case 3 Which one of the following laboratory/baseline monitoring parameters also needs to be obtained because amiodarone is being initiated? A. LFTs.B. CBC.C. Lipid panel. D. Electrolytes.
Type IV Agents • Dihydropyridine CCBs: • no significant antiarrhythmic effects • Non-dihydropyridine CCBs: • verapamil, diltiazem • block L-type Ca2+ channels • slow conduction, prolong refractoriness • ↓ SA/AV node automaticity
Type IV Agents • Non-dihydropyridine CCBs: • effective for SA/AV node automatic or reentrant tachycardias • slow AV conduction • help exercise induced tachycardias • benefits for tachycardias caused by triggered automaticity
Case 4 An 82-year-old woman with a medical history of atrial flutter, heart failure New York Heart Association (NYHA) functional class III (continually in and out of the hospital for exacerbation), and hypertension. The last time this patient was seen in the clinic, the decision was made for the patient to undergo ablation of atrial flutter. The patient cancelled the procedure because her family did not believe it was a good idea. The physician would like to initiate dronedarone.
Case 4 Which one of the following statements would explain why you disagree with the use of dronedarone in this patient? • Dronedarone should not be consideredan option for this patient because it is not approved for the treatment of atrial flutter. • Dronedarone should not be considered an option for this patient because the patient has hypertension. • Dronedarone should not be consideredan option for this patient because she has NYHA functional class III heart failure and frequent exacerbation. • Dronedarone should not be considered an option for this patient because it is better used in patients with NYHA functional class IV.
Dronedarone • MOA: Na+, K+, Ca2+ channel blocker, β-blocker • PK: Half-life 13-19 hours • CIs: QTc≥0.5 sec or PR≥0.28 sec, HF NYHA IV or recent HF exacerbation NYHA class II-III, severe hepatic impairment, second- or third-degree heart block, heart rate < 50 beats/min • DIs: CYP3A4 inhibitors, QT-prolonging agents, P-glycoprotein substrates • Decrease dose of digoxin by 50% • Monitor for myopathy with statins
Dronedarone • Dosing: • AF conversion/AF maintenance: • 400mg PO twice daily • Food helps increase absorption
Case 4 An 82-year-old woman with a medical history of atrial flutter, heart failure New York Heart Association (NYHA) functional class III (continually in and out of the hospital for exacerbation), and hypertension. The last time this patient was seen in the clinic, the decision was made for the patient to undergo ablation of atrial flutter. The patient cancelled the procedure because her family did not believe it was a good idea. The physician would like to initiate dronedarone.
Case 4 Which one of the following statements would explain why you disagree with the use of dronedarone in this patient? • Dronedarone should not be consideredan option for this patient because it is not approved for the treatment of atrial flutter. • Dronedarone should not be considered an option for this patient because the patient has hypertension. • Dronedarone should not be consideredan option for this patient because she has NYHA functional class III heart failure and frequent exacerbation. • Dronedarone should not be considered an option for this patient because it is better used in patients with NYHA functional class IV.