Download
1 / 71
721 likes | 1.32k Views
The Throwing Athlete’s Elbow. AHD May 31 st , 2012. Sasha Carsen JW Pollock G Wilkin. Goals/Agenda. Review Anatomy & Biomechanics Pathoetiology /Pathoetiomechanics Relevant Clinical Diagnoses Management Cases & Q’s. Anatomy. Medial Collateral Ligament (UCL/MUCL/TJL)

E N D
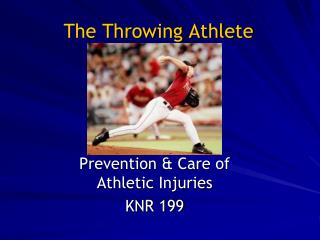
The Throwing Athlete’s Elbow AHD May 31st, 2012 Sasha Carsen JW Pollock G Wilkin
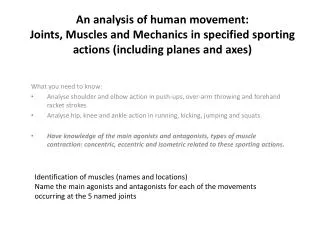
Goals/Agenda • Review Anatomy & Biomechanics • Pathoetiology/Pathoetiomechanics • Relevant Clinical Diagnoses • Management • Cases & Q’s
Anatomy Medial Collateral Ligament (UCL/MUCL/TJL) • Anterior Bundle • Strongest (260 N) • Primary Valgus stabilizer • Posterior Bundle • Transverse Bundle
Anterior Bundle O: anteroinferior medial epicondyle I:sublimetubercle ~18mm distal to coronoidtip - Isometric
Valgus Stability • Ulno-Humeral (olecranon-trochlea) primary at <20 & >120 • Anterior Bundle MCL is primary in between
Muscles • Flexor-pronator mass • Dynamic secondary stabilizers to valgus stress • Protect UCL • FCU may be most important due to synergistic position • Limited ability to compensate for MCL deficiency Davidson et al., AJSM 1995
A Recurring Theme:Valgus & Extension • Image valgus elbow
Windup • Weight to trailing leg, lead leg flexes • Trunk rotates away from target • Elbow flexed • Forearm pronated • Ends when ball leaves glove hand
Early Cocking • Stride initiation • Lead leg and hip drive toward target • Shoulder abduction and ER • Elbow extension controlled eccentrically • Ends when lead foot contacts ground
Late cocking • Shoulder abduction to 90° and ER to maximum (150-180°) • Elbow flexes to ~90° • Forearm pronates • Leading leg decelerates and pelvis rotates toward target • L-spine lordosis increases shoulder ER • Ends at max shoulder ER
Acceleration • Humerus rapidly transitions to IR, propelled by body rotation • Trunk flexes, elbow extends • Acceleration ~600,000 deg/sec2 • Max varus torque ~64 N⋅m • Ends with ball release
Deceleration/Follow-through • Nearly equally rapid deceleration (~500,00 deg/sec2) • Arm continues into horizontal adduction, shoulder IR, elbow extension • Posterior shoulder girdle muscles, cuff/deltoid, & elbow flexors decelerate arm • Weight transfer to lead leg
Throwing E - Risky Activities • Baseball pitchers • Multiple leagues, • all-star teams • Year-round • Javelin (or spear) throwers • QB • Etc.
Danger Zone Late Cocking & Early Acceleration
Late Cocking & Early Acceleration • That’s the one you need to remember! • Think Transition point • Late Cocking I put this off for way too long… Not to be confused with….
Again… • Image valgus elbow
DDx – A spectrumOften not in isolation! • Valgus Instability • MUCL • Acute (?) • Chronic • Valgus-Extension Overload • Postero-medial Impingement • Posterior Impingement • Loose Bodies • Ulnar Stress # • Medial Epicondylitis • Ulnar Neuropathy • OCD • Little Leaguer’s Elbow
History • Sporting history • Level of play, changes in routine, pitch count… • Acute/Chronic/A-on-C injury? • ?Pop • What phase brings out pain? • Late cock vs. follow-through/extension • Quality of pain? • NeuroSx? • Mechanical Sx? • ROM? • Changes in velocity, accuracy?
PE • Also check Shoulder/Scapula, compare sides • Carrying angle in pitchers can be >15deg • AROM/PROM • Mech block? MechSx? Ulnarnsublux? • Palpate MCL (sens, not spec) • Valgus Stress Test, Milking, and the Moving Valgus Stress Test • MVST = key, 100% sens, 75% spec
Imaging • XR • AP, Lat • Obliques • Postero-medial view • MRI • MRI vs A • Dependant on institution and radiologists, as well as clinical suspicion • Ligament vs Cartilage
Pathologies & Treatments MCL • Non-op • Sprain • Switch positions or drop sport • Not willing to commit to full year of Rehab • Kids should start with a non-op course, early ROM and pro/flex strength • Depending on level of play, prospects, risk/benefit, can consider Recon
MCL Repair Acute Rupture • Only indication is clear acute history • Good tissue on MR • Drill vs Anchors
Tommy John Procedure • Created & described by Jobe • Figure 8 Graft through bone tunnels +/- UlnarTranspo Modified to leave flexor O intact, now muscle splitting
Docking Method (Altchek) • Difference is on humeral side • More bone left intact • Tension @ 30deg (where MCL takes over as stabilizer) • Altchek does not routinely transpose ulnarn
Hybrid/Interference - DANE • Interference on Ulna • Dock vs interference on Humerus
Tommy John • 7th most wins for L-hander • Known for ‘sinker’ • Tommy John surgery in Sept ’74 with Dr. Frank Jobe, ’75 rehabbin’, back to MLB in ’76 • Went on to play until ‘89, winning another 164 games
Valgus Extension Overload • Most pitchers have some degree • Develop Postero-medial or Posterior Degenerative changes • Osteophytes • Loose bodies
Pathoetiology • High force and chronic laxity • Strongly correlated with chronic MCL pathology • Decr ROM, pain through follow-through
VEO - Tx • Non-op • Rest • NSAID’s • Cortisone • OR • Osteophyte excision • How much to take?? • Controversial, but in Thrower: • Only Pathological bone! (phytes) • Beware micro-laxity
Ulnar Stress # • Tx as per usual stress # • Early – Rest • Displaced or complete, must be reduced • Open vs. Scope and mini
Medial Epicondylitis • Not truly an epicondylitis, but rather tendinopathy of Flexor-Pronator mass • Non-op is mainstay • Rest, NSAIDs, Cortisone • PE • In high level athletes having concomitant surgery • Consider debridement, some use PRP (?evidence)
OCD • Remember, while medial side is under tension, lateral is under compression • In the child, must differentiate from Panner’s • Panner’s thought to be similar to LCP • <11yo • Prognosis excellent with Dx & Rest
Panner’s Fragmented, “ruffled” border - Lucencies& irregular ossification - Subchondrallucency - Usually heals with consolidation +/- residual capitellar flattening
OCD of Capitellum/Radial Head • More likely > 12 • Chronic micro-trauma • Prognosis poor if not caught early • As with any OCD lesion, prognosis improves with open Growth plates
OCD Mgt • Early or Open Physes • Rest • Later – depends on: • Size, stability & location of lesion(s) • Open results not great • Arthroscopic • Debridement & abrasion/MF • Fixation • OATs • Outcomes appear to be generally improving significantly
Little Leaguer’s Elbow • A spectrum of Medial EpicondyleApophyseal Injury • Apophysitis • Stress # • Displaced # • MCL is intact • Medial epicondyleapophysis closes around 15 years
Management • Prevention, prevention, prevention • Undisplaced • Rest. • Displaced • Literature typically says fix if >2mm displaced • Andrews says in the high level kid fix if ANY displacement, and get anatomic
Conclusion • Understand, isolate, and treat the pathology • Know the patient’s goals • This often means more than one pathology • Rest plays a very significant role in the prevention, treatment, and rehab of throwing elbow injuries Homer Simpson, on watching baseball while sober: • “I never realized how boring this game is…”
Last Time… • Image valgus elbow
Valgus Instability • MUCL • Acute (?) • Chronic • Valgus-Extension Overload • Postero-medial Impingement • Posterior Impingement • Loose Bodies • Ulnar Stress # • Medial Epicondylitis • Ulnar Neuropathy • OCD • Little Leaguer’s Elbow