Download
1 / 12
120 likes | 159 Views
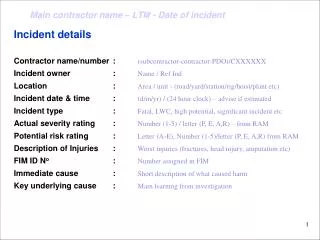
Incident details Contractor name/number : (subcontractor-contractor-PDO)/CXXXXXX Incident owner : Name / Ref Ind Location : Area / unit - (r oad /yard/station/rig/hoist/plant etc) Incident date & time : (d/m/yr) / (24 hour clock) – advise if estimated

E N D
Incident details Contractor name/number : (subcontractor-contractor-PDO)/CXXXXXX Incident owner :Name / Ref Ind Location : Area / unit - (road/yard/station/rig/hoist/plant etc) Incident date & time : (d/m/yr) / (24 hour clock) – advise if estimated Incident type : Fatal, LWC, high potential, significant incident etc Actual severity rating : Number (1-5) / letter (P, E, A,R) – from RAM Potential risk rating : Letter (A-E), Number (1-5)/letter (P, E, A,R) from RAM Description of Injuries :Worst injuries (fractures, head injury, amputation etc) FIM ID No: Number assigned in FIM Immediate cause : Short description of what caused harm Key underlying cause : Main learning from investigation
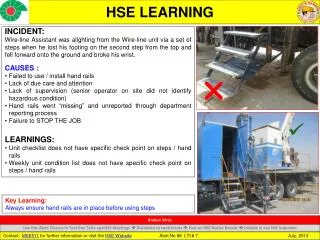
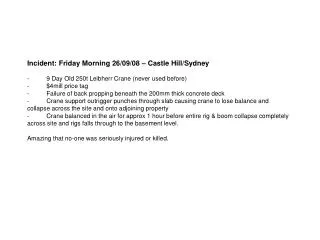
Description of the incident: • This should include the relevant facts explaining what happened including all relevant parties • Leading up to the incident • Immediately before the incident • During the incident • Immediately after the incident • In the emergency escalation of the incident • Important Note: • This should be in sufficient detail to allow a person who does not know anything about the incident to imagine it. It should only be about what happened and not why it happened. Do not include investigation findings here, simply describe the incident as the investigation has shown it happened. • For complex incidents involving the interaction of several different parties, a timeline can be added on a separate slide immediately after this one.
Photographs, diagrams & sketches • Rules • Only include photos or sketches if they add value explaining the incident or causes. • Each photo/sketch must be labeled to explain what it is and why it has been shown. • Ensure photos are labeled to explain context (e.g. road looking in direction of; historical photo of plant before fire etc). • Ensure all photos are evidenced to the investigation. (have formed part of the investigation) • Ensure all photos are of suitable clarity. • Include a maximum of four photographs/sketches per page. • Do not exceed three pages of photographs, diagrams and sketches
Key investigation findings: • The findings should be listed in terms of subject and importance – (list below is non-exhaustive) • People, • training, age, experience, nationality, medical conditions, disciplinary record etc • Equipment, • type, serial number, maintenance, inspection, failings, appropriate for use etc • Activities at the time of the incident, • lifting, driving, commuting, drilling, POOH etc • Relevant environment, • workplace conditions, weather, lighting, floor surface, dust, cramped etc • Operational management , • supervision, TBTs, SJPs, SWPs, STOP, availability on site etc • Contractual management, • audits, CH involvement, defaults, inspections, visits, issues, sub contractor management • HEMP, • review, appropriateness to the incident, is it used, how is it translated into action • Previous relevant incidents/learnings, • what, where, were they aware of it, were controls introduced • Emergency response, • how effective was it, did it impact on the severity?
Conclusions: Active causational failures: The acts or conditions precipitating the incident. They usually involve the front-line staff, the consequences are immediate and can often be prevented by design, training or operating systems. Latent causational conditions: Managerial influences and social pressures that make up the ‘way we do things around here’, influence the design of equipment or systems and define supervisory inadequacies. They tend to be hidden until triggered by an event. Latent conditions lead to human errors or violations. Latent causational management failures (underlying causes): Latent failures are due to people removed in time and space from the operation, e.g. designers, decision makers and managers. Latent failures are typically failures in the HSE- MS (design, implementation or monitoring). e.g: poor design of plant/equipment; ineffective training or communications; inadequate supervision or resources; uncertainties in roles and responsibilities. Latent failures are usually hidden until they are triggered by an event likely to have serious consequences. Did the HSE–MS identify these hazards and place barriers for mitigation? If not, then it is a latent management failure
Feedback to Incident Owner: (Depth, accuracy, quality, robustness, feasibility and appropriateness of investigation findings and recommendations) … … … Query raised: (raise questions which have not been adequately answered in the investigation or presentation) ... … … Additional recommendations: (Including, revisiting the investigation to improve quality, adding any key recommendations that are requested by the directorate management but have been missed in the investigation, or removing inappropriate recommendations) … … … • Directorate IRC Minutes: Date held: (d/m/yr)
Non-causational findings but worthy of note: (Investigations can often identify issues which although not directly linked to the cause of the incident are important to report, correct and communicate for wider learning. List these here in bulleted format.)
Tripod Tree (include copy of the Tripod tree flow diagram for all 4/5 incidents or High Potential) Investigation reports requiring a Tripod must confirm that the findings and recommendations match the Tripod findings
Immediate actions: (Report all remedial measures actions taken and completed within one week of the incident) ... ... • Redline recommendations: • Report the five most important actions to prevent a reoccurrence in the future. • Note: • Causations to be linked with the recommendations, noting that one causation may have one or more recommendations • Recommendations to include title of Action Party and not just PDO or Contractor Company. These must be under separate columns – one each for PDO and for Contractor • Actions to be given to PDO and or direct contractors only. The sub-contractor to be indicated as action party in brackets • Where an action is with a contractor the corresponding PDO action party is the Contract Holder to ensure it is completed & in FIM
Additional Recommendations: • (include the less urgent actions required to improve the management and for other contractors to learn from) • Note: • Causations to be linked with the recommendations, noting that one causation may have one or more recommendations • Recommendations to include title of Action Party and not just PDO or Contractor Company. These must be under separate columns – one each for PDO and for Contractor • Actions to be given to PDO and or direct contractors only. The sub-contractor to be indicated as action party in brackets • Where an action is with a contractor the corresponding PDO action party is the Contract Holder to ensure it is completed & in FIM Contact CEO & PDO Director joint statement _________________________ _____________________ Contractor CEO PDO Director (RESPONSIBLE) (ACCOUNTABLE)
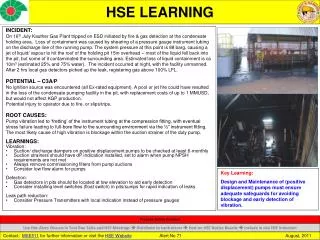
PDO safety advice • Date: Incident title • What happened? • Very short description of what happened • Your learning from this incident.. • ( This must relate to the people at risk of harm or people at risk of causing the harm) • Title (e.g. Drivers) • Learning points for them from the investigation Photo explaining what was done wrong Photo explaining how it should be done right Strap line – (keep short and punchy
Management learnings • As a learning from this incident and ensure continual improvement all contract • managers are to review their HSE HEMP against the questions asked below • Confirm the following: • Make a list of closed questions (only ‘yes’ or ‘no’ as an answer) to ask other contractors if they have the same issues based on the management or HSE-MS failings or shortfalls identified in the investigation. Pretend you have to audit other companies to see if they could have the same issues.