Download
1 / 98
980 likes | 1.01k Views
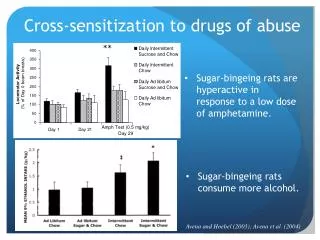
Central Sensitization. Denise Jagroo London 2016. WHY?. Why do all my pelvic pain patients seem just like…. ME?. Why???. ???. Its like playing whack-a-mole. About Denise. New York University: Undergraduate and Graduate Doctorate in Physical Therapy 2002 Manual Therapy Certification

E N D
Central Sensitization Denise Jagroo London 2016
WHY? • Why do all my pelvic pain patients seem just like…. ME?
About Denise.. New York University: Undergraduate and Graduate • Doctorate in Physical Therapy 2002 • Manual Therapy Certification • University of St. Augustine
About Denise… • Certificate of Achievement in Pelvic Physical Therapy • American Physical Therapy Association Women’s Health Section • Board Certified Specialist in Women’s Health • American Physical Therapy Association Women’s Health Section
About Denise…. • Established a Pelvic Rehab Clinic at the Manhattan Veteran’s Hospital 2009 • Owner of Private Practice In New York • Staten Island • Denise Jagroo Physical Therapy
About Denise Lecture nationally and internationally to health clinicians regarding Pelvic Health and Rehabilitation
About Denise… • Author: • “Your Best Pregnancy” • Host Webseries on YouTube • Exercise equipment • Blogger
Sensitization • Before we talk about central sensitization, what is sensitization? • Sensitization- an increase in the excitability of neurons, so they are more sensitive to stimuli or sensory inputs • Natural physiological response to help us avoid pain
What? Sun Burn!
What is Central Sensitization? • Type of neuronal plasticity (woolf , 2007) • Activity-dependent synaptic plasticity in the spinal cord that generates post-injury pain hypersensitivity
HUH? • The connection between neurons can CHANGE in strength! • Either due to using it too much or using it too little
Abnormal Changes in the CNS Peripheral Input Hypersensitive painful and prolonged response (fibromyalgia)
Central Sensitization • Benign inputs begin to produce painful responses. • Or worse, no input, such as phantom limb pain.
What is Central Sensitization? Simply put: An amplification of neural signaling within the CNS that elicits pain hypersensitivity - (Woolf 2007)
Ok, so far… • Not as simple as we thought • There are changes that can happen in the CNS • Can change the effect of a stimulus • Remember to think of our patients…
? • Injury • Afterwards it doesn’t take as much to make someone say ‘ouch!’ • Something seems more painful than it should be…
By the 1980s.. • Realization that synapses were subject to a form of use-dependent plasticity that could increase their strength or efficacy
? • Stim • Then NO STIM! • But still feeling the effects!! Even after stim taken away!
Neural windup? • NO! • This phenomenon (central sensitization) differed from windup, which represented a progressively increasing output during the course of a train of identical stimuli
In simple terms… Central sensitization: • Pain that’s more intense = (Hyperalgesia) • Pain where there shouldn’t be pain = (SecondayHyperalgesia) • Pain from something that shouldn’t be painful = (Allodynia)
Central Sensitization Skin Effects LaMotte 1991 & 1992 -1% Intradermal Capsaicin injections in humans - in receptive field of peroneal nerve (below knee) studied via subcutaneous microelectrode -TRPV1 (detection/regulation of body temp, sensation of scalding heat/pain)
Central Sensitization • Injection Site: • Intense pain lasting minutes (at injection site) • 3 zones: heat hyperalgesia 1-2 hours • Dynamic tactile allodynia: several hours & beyond heat area • Largest zone to pinprick—WAY OUTSIDE—24 HOURS
Biomarkers • FMRI: Functional magnetic resonance imaging or functional MRI (fMRI) is an MRI procedure that measures brain activity by detecting associated changes in blood flow
Biomarkers • Increased excitability of neurons in somatosensory cortex evoked by low threshold aB stim within secondary hyperalgesia • Brainstem changes • Cerebral processing
Visceral Effects Brock 2010 • GI Tract: esophageal stim thermal & mechanical pain hypersensitivity in RECTUM
Again… Central sensitization: • Pain that’s more intense = (Hyperalgesia) • Pain where there shouldn’t be pain = (SecondayHyperalgesia) • Pain from something that shouldn’t be painful = (Allodynia)
Cross-Talkin’ • GOOD: Close neural connections in the sacral spinal cord are ESSENTIAL complex coordinated visceral functions in the pelvis • BAD: Intimate connections also allow neuroinflammation to spread from involved to uninvolved neurons via dorsal horn
Viscero-somatic reflexes • Visceral somatic reflexes: afferent stim from a visceral source can affect somatic structures • Nerve cell bodies in dorsal horn of spinal cord and other CNS regions receive convergentinput from both somatic and visceral structures
Viscerovisceral & Viscerosomatic Convergence (Di Saia 2012) • Afferent signals converge —aberrant interactions that can result In painful sensations from organs that are not directly inflamed or stimulated (cross-talk) and from nearby somatic structures (cross-sensitization)
Viscerovisceral & Viscerosomatic Convergence The concept of viscerovisceral & viscerosomatic convergent helps explain why there is so much overlap in the presence of conditions such as • endometriosis • Interstitial Cystitis (PBS) • IBS • Vulvodynia
Cross –Talkin’ • End terminal stimulatedsubstancePretrogade traveling down C andA delta fibersincreased expression of sodium channels & sensitization distally at the terminal nociceptors PAIN organ system to organ system & spread of pathologies • Central connection
Cross Talkin’ • Noxious Prodromic • (PeripheralCentral) noxious afferent stim from an irritated pelvic organ leads to
Cross-Talkin’ • Andromic (CentralPeripheral) • Afferent stim & co-sensitization of another non-irritated pelvic organ
Cross-Talkin’ • Reflexive pathways may occur: • Locally via axon collaterals (dichotomizing afferents) • Spinal cord (DRG) • CNS
Cross Talkin’ • SOOooooo… • Neuroinflammation via andromicpathwaysfunctional changes in the Uninsultedorgan with little or no evidence of an organic etiology