Download
1 / 15
150 likes | 1.27k Views
Brachial Plexus Injuries. Chapter 11 Athletic Injury Assessment. Clinical Anatomy p.371. Innervation for upper extremity Levels--fig.11-5, .371 C 5- T 1 nerve roots Upper trunk:C5-C6 Middle trunk: C7 Lower trunk: C8-T1. Brachial Plexus Pathology. “Burners” or “Stingers”

E N D
Brachial Plexus Injuries • Chapter 11 • Athletic Injury Assessment
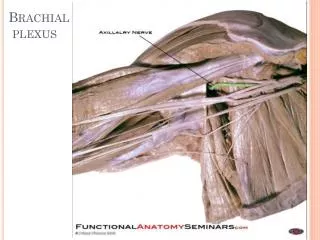
Clinical Anatomyp.371 • Innervation for upper extremity • Levels--fig.11-5, .371 • C5-T1nerve roots • Upper trunk:C5-C6 • Middle trunk: C7 • Lower trunk: C8-T1
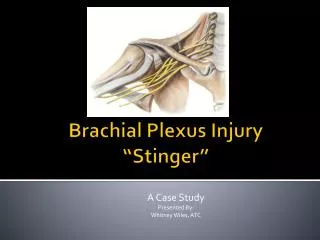
Brachial Plexus Pathology • “Burners” or “Stingers” • Nerve stretch or compression • FB: more common in defensive players • Assess all dermatomes C5-T1 in assessment • Table 11-6, p. 386
Brachial Plexus Pathology—p. 385 • Mechanisms: • acute onset • traction/stretch • compression • fig. 11-16, p. 385 • Symptoms: • burning/tingling in upper extremity • weakness in UE
Brachial Plexus Pathology • Other considerations: • cervical spine injury • cervical stenosis • Rule out other injuries • No clearance until all symptoms resolve completely
Brachial Plexus Pathologyp.387 • Assessment: • Brachial plexus traction test-- • p.387 • Box 11-5, p. 387 • 2 possible results • Possibly (+) Spurling test • Dermatome testing
Brachial Plexus Myotomes • C5: shoulder abd./ER • C6: elbow flex.; wrist ext • C7: elbow ext.; wrist flex. • C8: finger flex. • T1: finger abd.
Brachial Plexus Injury: Treatment • Remove from contact • Test/Retest • Rule out other pathologies • Bilateral weakness • Weakness outside brachial plexus (shoulder shrug)
Brachial Plexus Injury: Return to Play Guidelines • Full painfree AROM in UE and neck • Normal sensation • Correction of technique/ equipment to prevent re-injury
Cervical Stenosis • Signs/Symptoms: • recurrent stingers • bilateral complaints • proper technique • neurological signs outside of brachial plexus • transient quadriplegia • usually congenital problem
Cervical Stenosis • Cervical spinal canal usu. 14.5mm-20mm(C3-C6) • CSF coats and cushions spinal cord • small canal or large cord may = stenosis • Medical imaging used to measure risk
Cervical Stenosis: Assessment • Torg Ratios • VB=SC (+/- 20%)=NL • C4-C6 • original research did not include FB players • 1990--33% of NFL had stenosis • stenosis=ratio BUT • ratiostenosis • Imaging • x-ray (magnification) • CT Scan/MRI • Contrast CT • C-spine vs whole spine
Cervical Stenosis: Management • Symptoms dictate workup • Imaging: • x-rays to determine Torg ratio • If Torg ration outside of NL ranges (.8-1.2) then CT/MRI • whole spine imaging?
Cervical Stenosis: Management • Return to Play • Assess risks based on imaging/ratios • Assess possible technique changes • if stenotic-avoid all sports which threaten the C-spine
Burners vs. Stenosis • Burners • One-sided • Acute • Strong cause-effect • Limited to brachial plexus only • Normal imaging • Normal Torg ratio • Stenosis • Bilateral • Chronic • Poor cause-effect • Extends beyond brachial plexus • Abnormal imaging • Abnormal Torg ratio