Download
1 / 24
350 likes | 1.89k Views
Carotid Cavernous Fistula. Laura S Gilmore, MD Department of Ophthalmology TTUHSC February 13, 2004 Discussant: Kenn Freedman, MD. Case Presentation. 26yo AAM s/p MVA CHI, L zygoma fracture Consulted for proptotic, red OS

E N D
Carotid Cavernous Fistula Laura S Gilmore, MD Department of Ophthalmology TTUHSC February 13, 2004 Discussant: Kenn Freedman, MD
Case Presentation • 26yo AAM s/p MVA • CHI, L zygoma fracture • Consulted for proptotic, red OS • CT: proptosis OS. No basilar skull fracture. no retrobulbar hematoma, no superior ophthalmic vein enlargement, no ocular muscle enlargement
Differential Diagnosis Cavernous Sinus Thrombosis • Retrobulbar Hematoma • Unrecognized intra-orbital FB, with possible cellulitis • Carotid Cavernous Sinus Fistula • Tumor
Physical Exam • General: sedated, intubated • Lids: edematous, margins intact • Pupils: 2.5mm->2mm, 7->NR • Conj: chemosis, OS>OD; SCH OS • IOP: 16, 28 • Cornea 2+ edema OS, clear OD • + gross proptosis OS • + bruit OS on auscultation, no neck bruit • DFE: discs flat with sharp edges, vessels normal, retina flat OU
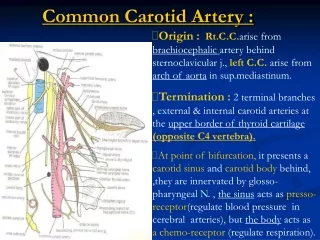
Carotid Cavernous Fistula • Abnormal communication between previously normal carotid artery and cavernous sinus • Characterized as: -Direct vs. Indirect -High vs. Low Flow -Traumatic vs. Spontaneous
Mechanisms of CCSF • Trauma • Spontaneous causes: • rupture of intracavernous aneurysms • neurofibromatosis • atherosclerotic disease • collagen vascular disease • Iatrogenic
Direct Carotid Cavernous Fistula • Arterial blood passes directly through a defect in the wall of intracavernous portion of ICA • Blood in vein becomes arterialized • Venous pressure increases • Arterial pressure and perfusion decreases
Signs of Direct CCSF • Ptosis • Very red, chemotic conj • Increased IOP from increased episcleral venous pressure • Anterior segment ischemia in 20% • Corneal edema, cell/flare, iris atrophy, rubeosis, cataract • Proptosis is pulsatile • Bruit and thrill • Muscle palsies • Visual loss
Etiologies of Direct CCSF • From trauma in 75% of all cases • Basal skull fracture tears ICA within cavernous sinus • Traumatic fistulae-high flow rates, sudden and dramatic onset of symptoms • Spontaneous rupture of aneurysm or atherosclerotic artery in 25% • Post-menopausal, hypertensive females • Lower flow rates, less severe symptoms
Mechanisms of Traumatic CCSF • direct injury from basilar skull fracture • injury from torsion or stretching of the carotid siphon upon impact • impingement of the vessel on bony prominences
Indirect Carotid Cavernous Fistula • Fistulous connection is within the wall of the cavernous sinus • Tend to be low-flow • Small meningeal arteries supplying dural wall of cavernous sinus can rupture spontaneously, while ICA itself remains intact • Insidious onset, mild orbital congestion, proptosis, low or no bruit • Lesions may fluctuate, and may resolve spontaneously
Clinical Presentation of CCSF • Ophthalmic consequences of CCSF are caused by compression and ischemia related to increased venous pressure and reduced arterial pressure • flow reversal leads to engorged ophthalmic veins causing proptosis, conjunctival injection, chemosis. • Patients complain of retro-orbital headache, or a bruit. Facial pain with V1 and V2 involvement
Clinical Presentation of CCSF • Other manifestations: • congestion of the opposite orbit • diplopia • ptosis, mydriasis • corneal ulceration • loss of visual acuity • transient neurological deficits • subarachnoid hemorrhage
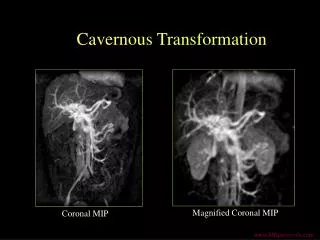
Radiological Evaluation of CCSF • Angiography is the definitive diagnostic examination • CT and MRI may show • Enlarged superior ophthalmic vein • Enlarged muscles • Enlarged cavernous sinus with a convex shape to the lateral wall
Treatment of CCSF • Most are not life-threatening • Only involved eye is at risk typically • Main indicators for treatment • Glaucoma • Diplopia • Intolerable bruit or HA • Severe proptosis causing exposure keratopathy • Spontaneous closure from thrombosis of cavernous sinus is unlikely (as in trauma, high-flow)
Treatment of CCS Fistulas • 99% of treatment is done by interventional neuroradiologists • Intravascular approach-placement of thrombogenic materials, eg coils • Other therapies include: • carotid artery ligation • surgical exposure with clipping of the fistula
Summary • Direct CCSF usually results from trauma • Patients typically present with proptosis, conjunctival injection, and a bruit • Angiography when pt stable • Transarterial embolization