Download
1 / 20
200 likes | 433 Views
Carotid Surgery. Anesthetic considerations Sam Hemans MD DDS Charles Smith MD 3 August 2004. Objectives. Pathophysiology of carotid dz Strategy for anesthetic evaluation Perioperative management Complications New therapies in the field. Epidemiology.

E N D
Carotid Surgery Anesthetic considerations Sam Hemans MD DDS Charles Smith MD 3 August 2004
Objectives • Pathophysiology of carotid dz • Strategy for anesthetic evaluation • Perioperative management • Complications • New therapies in the field
Epidemiology • 1.2m strokes or tia’s each yr in the US • >150,000 deaths each yr • 3rd leading cause of death • CEA introduced in 1954 as a preventive measure for occlusive dz.
Indications • >70% in symptomatic patients • 50- 69% in symptomatic patients with low risk • >60% in asymptomatic patients with favourable surgical risks
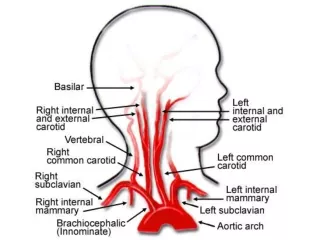
Physiologic considerations • Carotid dz is due to atheroslerosis • Most common site is the bifurcation of vessels • Ischemia is often due embolic phenomenon • During ischemia collateral flow critical • Principal pathways : Circle of Willis,extracranial anastomotic channels,leptomeningeal communications
Preoperative evaluation • CEA has an inherent risk of perioperative stroke and cvs events • 25% strokes associated with CEA occur intra-op • 33% mostly embolic; some hemodynamic in origin • Recent data from the NASCET reports a 6.5% rate of stroke and death • 1.1% rate of death, 0.9% disabling stroke,4.5% disabling stroke • Increased risk for stroke is most strongly associated with an active neurologic process prior to surgical intervention
Preoperative evaluation • Other risk factors for poor neurologic outcome • Hemispheric vrs retinal tia’s • Left sided procedure • Ipsilateral ischemic lesion on ct • Contralateral carotid occlusion • Impaired consciousness • Poor collaterals • An irregular or ulcerated plaque • Cea with CABG
Pre-op • Medical complications occur 10% of time • Hypertension: incidence of neurologic deficit related pre-op uncontrolled HTN • Multicenter study , diastolic>110 predictor of adverse events • Reasonable recc is delay elective surgery for diastolics>110 • A less firm recc is to delay elective sx for sys >180 • Carotid dz is a manifestaton of systemic dz: Good cardiac hx, previuos mi,angina,exs tolerance,chf,arrhythmias,ekg,cxr routine.Echo and stress test may be indicated as well. • Diabetes, may have increased cardiac related death but data seems to indicate that CEA can be performed safely in these patients • Renal Insufficiency, have a overall increased risk for stroke, death and cardiac morbidity
Monitoring • Std ASA monitors • Continuous lead II , V5 • Arterial line routine • PA cath and TEE may be considered in patients with symptomatic dz or recent mi
Anesthetic Management • No compelling advantage has been demonstrated with either regional or general anesthesia • Technique should optimize perfusion to the brain,minimize myocardial stress and allow rapid recovery • Choice is often strongly influenced by the surgeon’s preference and the anesthesiologist familiarity with a specific technique • Recent study, sevo and des provided quicker extubation times and recovery profiles after CEA c/w iso with no significant peri-op differnces in CI and ST segment analysis • Propofol and narcotics may be associated with hypotension
Regional technique • A regional technique for CEA necessitates the correct combination of patient, surgeon and anesthesiologist • CEA requires block of C2- C4. • Superficial cervical block, deep cervical, epidural and straight local or a combination of these have been utilized successfully
Regional technique • Tangkanakul et al performed a meta – analysis of studies evaluating the efficacy and safety of regional anesthesia • The non-randomized study suggested that the use of regional was associated with approx 50% reductions in the odds of stroke, death, mi, pulmonary complications and length of hosp stay. • There was far too little data to either confirm or refute the study.
Modalities of Cerebral Protection Surgical- placement of a shunt during x-clamp Physiologic: Mild hypothermia 33-34C Rx hyperglycemia Hypertension Hemodilution Maintenance of normocarbia Anesthetic:Barbiturates, no evidence for permanent focal deficits volatile anesthetics, iso and sevo associated with lower critical bf c/w halothane and enflurane Etomidate shown to worsen outcome in animal models,thio shown to improve ischemic injury Propofol , animal studies have produced mixed results
The objective is a smooth and prompt emergence with optimal systemic and cerebral hemodynamics, additional problems as follows: Hypertension Hypotension Myocardial Infarction Stroke, usually embolic Bleeding Cranial Nerve injury, occurs in 10% of patients The most commonly injured nerves are,hypoglossal nerve,vagus, recurrent laryngeal,accessory nerve. Unilateral damage usually no immediate sx or intervention Bilateral damage could result in upper airway obstruction Beware of patients with pre-existing neck surgery Post- op
CEA and CABG One of the more difficult decision matrices regards the patient who presents with simultaneous dz of the carotid and the coronary vessels Best available evidence – doubling of risk of death or stroke if performed as a single anesthetic as opposed to a staged procedure In a staged procedure risk is related to which procedure is performed first: If CEA is performed first the risk of mi increases; if CABG is performed first the risk of stroke increases
Timing of CEA after Stroke • Presently there is insufficient data to establish any guidelines • In the 1980’s CEA patients typically stayed in the ICU for1-2days then floor 3-5days • Recent data has shown that 24hr ICU IS sufficient since most perioperative strokes following CEA occurred within 24hrs after the surgery
Indications, symptomatic patients if stenosis>70% and for selected patients if the lesion is 50- 69% Pre-op concerns, uncotrolled htn Anesthetic technique no demonstrated advantage of regional vrs general Cerebral Monitoring, neurologic status in the awake patient, and the EEG may be considered close to the gold standard Post op concerns, usually due to htn Whichever anesthetic method is chosen, it is imperative that CBF be optimized, with min cardiac stress especially during x-clamping. The risk of ischemia may be decreased by maintaining normal to high perfusion pressure Summary
Carotid stenting and Angioplasty, the procedure involves the placement of a saline filled balloon,pre-loaded with a stent under angiographic guidance and applying 15atm for 3mins, anesthetic technique is sedation Drawbacks, profound bradycardia, high incidence of strokes from the angiography alone. SAPPHIRE (Stenting and Angioplasty with Protection at High-Risk for Endarterectomy) First randomized trial to evaluate the safety and efficacy of carotid artery stenting with emboli prevention in high surgical risk patients. High risk criteria included, prior cea, neck surgery, radiation to the neck, occlusion of the contralateral carotids, chf and other confounding medical problems New Therapies
Study actually a randomized trial which compared cea with stenting and angioplasty Enrollment terminated after 723 patients were enrolled, 416 registry and 307 randomized, as interim analysis showed a marked benefit in favour of stenting. Success defined as <30% residual stenosis 30 day periprocedural combined stroke/mi/death rate which was the study endpoint was 5.8% in the stent group but 12.6% in the surgical group SAPPHIRE study Showed that in high risk patients CAS was a superior to CEA and that emboli prevention was also improved in the CAS group of patients. conclusion