Download
1 / 53
530 likes | 673 Views
Learn about the internal, external branches, and common variants of carotid and vertebral arteries. Explore neurovascular syndromes and artery segments.

E N D
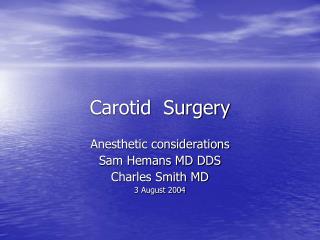
Towne Carotid Lateral Carotid 1. Internal Carotid2. External Carotid3. Anterior Cerebral4. Middle Cerebral
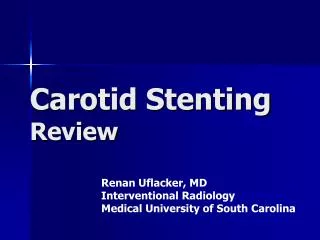
Towne Vertebral Lateral Vertebral 1. Vertebral2. Posterior Inferior Cerebellar3. Basilar4. Superior Cerebellar5. Posterior Cerebral6. Occipital7. Posterior Temporal 1. Vertebral2. Posterior Inferior Cerebellar3. Anterior Inferior Cerebellar4. Basilar5. Posterior Cerebral
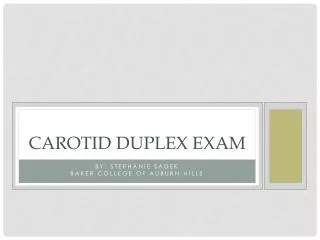
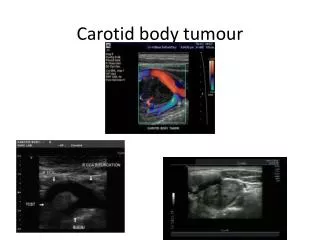
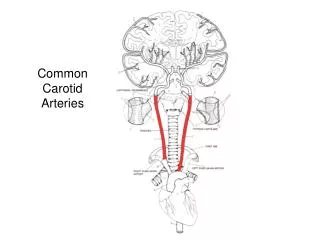
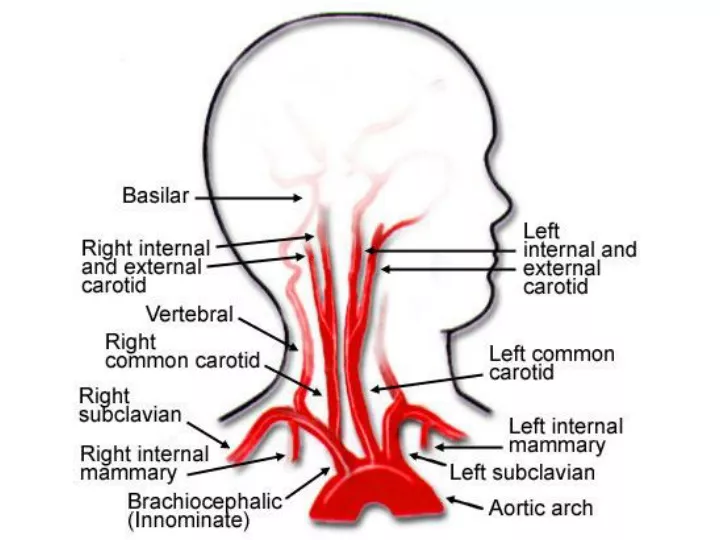
Carotid arteries (red arrows) and vertebral arteries (yellow arrows) in neck
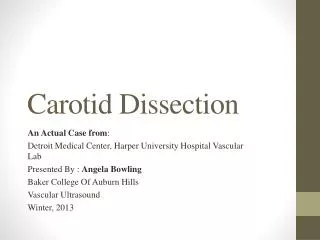
Common (blue arrow), Internal (red arrow), and External (yellow arrow) branches of the Left Carotid Artery
Common normal variants include hypoplasia of one or both posterior communicating arteries, a hypoplastic or absent A1 ACA, and fetal origin of PCA from ICA.
MR venogram - sagittal view [rght image]; A = Lateral (transverse) sinus; B: Sigmoid sinus C = Confluence of sinuses; D = Superior sagittal sinus; and E = Straight sinus.
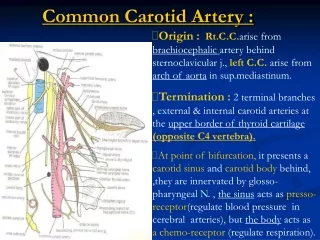
Internal Carotid Artery Begins at the bifurcation of the Common Carotid Artery (level of C4). Terminal branches: ACA and MCA. Four segments: cervical, petrous, cavernous, and supraclinoid
Supplies most of the medial surface of the cerebral cortex (anterior three fourths), frontal pole (via cortical branches), and anterior portions of the corpus callosum. • Perforating branches (including the recurrent artery of Heubner and Medial Lenticulostriate Arteries) supply the anterior limb of the internal capsule, the inferior portions of head of the caudate and anterior globus pallidus.
Bilateral occlusion of ACA at their stems results in infarction of the anteromedial surface of the cerebral hemispheres: • Paraplegia affecting lower extremities and sparing face/hands. • Incontinence • Abulic and motor aphasia • Frontal lobe Symptoms: personality change, contralateral grasp reflex. Unilateral occlusion (distal to Ant. Comm. origin) of ACA produces contralateral sensorimotor deficits mainly involving the lower extremity with sparing of face and hands (think of the humunculus).
From Internal Carotid Bifurcation to Anterior Communicating Artery. A1 Branches: Anterior Communicating Artery(connects both sides of anterior circulations). Medial Lenticulostriate Arteries (supply basal ganglia, anterior limb of internal capsule). Recurrent Artery of Heubner (supplies head of caudate and anteroinferior internal capsule).
Connects bilateral anterior circulations.Common location for cerebral aneurysms.
Supplies head of caudate and anteroinferior internal capsule.
Pericallosal Artery Continuation of the ACA as it arches superiorly and posteriorly.Supplies the medial surface of the cerebral hemispheres and corpus callosum.
Supplies most of the temporal lobe, anterolateral frontal lobe, and parietal lobe. Perforating branches supply the posterior limb of the internal capsule, part of the head and body of the caudate and globus pallidus.
Unilateral occlusion of MCA at the stem (proximal M1 segment) results in: • Contralateral hemiplegia affecting face, arm, and leg (lesser). • Homonymous hemianopia - Ipsilateral head/eye deviation. • If on left: global aphasia. • Usually occlusion is embolic in nature - thrombotic occlusion more common in carotids.
Branch of M1 Segment of MCA. Supplies basal ganglia structures: Part of head and body of caudate, globus pallidus, putamen, and the posterior limb of the internal capsule.
Sylvian (M2) Segment MCA Segment divides into superior and inferior divisions which can be a site for an embolus to lodge.Branches supply: Temporal Lobe and Insular Cortex (sensory language area of Wernicke)Parietal Lobe, (Sensory cortical areas), Inferolateral frontal lobe.
NEUROVASCULAR SYNDROMESuperior Division Infarction:"Brachiofacial paralysis"Sensorimotor deficit involving face and arm, leg to a lesser extent. Foot is spared.Ipsilateral deviation of head/eyes.With Left lesion may have initial global aphasia -> motor aphasia.No impairment of alertness. Inferior Division Infarction:Superior quadrantanopia / homonymous hemianopia.LEFT lesion: Wernicke aphasia (deficit in comprehension of spoken/written language) RIGHT lesion: Left-sided visual neglect.
Cortical (M3) Segment MCA Distal branches of MCA course laterally to insular cortex and loop around operculum - "Candelabra" effect seen on lateral angiograms. Embolization of individual cortical branches can produce highly circumscribed infarctions accompanied by specific neurologic deficits.
Measurement locations along the vertebral artery (I–III) depicted on a contrast-enhanced MRA (left) and on a schematic image in relation to the bony anatomy (right)
Identify the following structures on the left that comprise the circle of Willis: Internal Carotid Artery Anterior Cerebral Artery Anterior Communicating Artery Posterior Communicating Artery Posterior Cerebral Artery Basilar Artery Middle Cerebral Artery Superior Cerebellar Artery Pontine Peforating Arteries
Posterior Cerebral Artery • The PCAs are paired vessels, usually arising from the top of the basilar artery and curving laterally, posteriorly, and superiorly around the midbrain. • The PCA supplies parts of the midbrain, subthalamic nucleus, basal nucleus, thalamus, mesial inferior temporal lobe, and occipital and occipitoparietal cortices. • In addition, the PCAs, via the posterior communicating arteries (PCOM), may become important sources of collateral circulation for the middle cerebral artery (MCA) territory.
Posterior Cerebral Artery • The PCA is divided into P1 and P2 segments by the PCOM. Penetrating branches to the mesencephalon, subthalamic, basal structures, and thalamus arise primarily from the P1 segment and the PCOM. These penetrating arteries include the thalamogeniculate, splenial (posterior paricallosal artery), and lateral and medial posterior choroidal arteries. • The P2 segment bifurcates into the posterior temporal artery and the internal occipital artery. The posterior temporal artery further divides into anterior, middle, posterior, and hippocampal branches. The internal occipital artery divides into calcarine and occipitoparietal branches.