Download
1 / 21
210 likes | 321 Views
Module 5.3. Recruiting consumers. The use of social marketing techniques and communication strategy. Presentation purpose. Target audience Health professionals and project workers on DPMI projects Aim To recruit consumers to DPMI programs Objectives

E N D
Module 5.3 Recruiting consumers The use of social marketing techniques and communication strategy
Presentation purpose Target audience • Health professionals and project workers on DPMI projects Aim • To recruit consumers to DPMI programs Objectives • Provide an overview of the issues in recruiting consumers • Explore the barriers and facilitators in engagement • Discuss consumer need and communication strategies
“We had a great program but we just couldn’t manage to recruit the consumer numbers we wanted…”
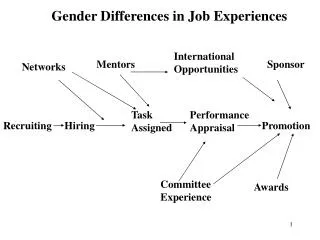
The ideal referral pathway Service Access A need for a service identified Service provider or friend asked for help Referral Intake, eligibility screening
The referral pathway maze!! Access Denied Don’t ask: isolated and disconnected Lack of follow through Don’t know where to turn Bad referral Redirected referral Ineligible for service Service Access A need for a service identified Service provider or friend asked for help Referral Intake, eligibility screening Can’t complete application process Green = Ideal pathway Service doesn’t exist or details changed Service provider unaware of appropriate service Access Denied Red = Diversion Cost, physical access, transport, language barriers
Characteristics Who? e.g. primary target – consumers, secondary target – service providers Demographics (e.g. age, where they live, gender, cultural background) Psychographics (e.g. how they live, mindset) Needs and experiences (e.g. qualitative research, consumer participation) Choose segments of the target group Can you drill the target group down further to make targeting easier? Who are your target group?
Does the program strategy fit with consumer needs? • Program / Service • What is the program / service? • Can people/agencies clearly identify with it (do they feel and acknowledge there is a problem)? • Are the benefits to the consumers/providers/agencies identified? • Are the people delivering the program consistent with consumer needs (e.g. service providers or consumers, how selected, trained and motivated)? • Is it a structured and validated program? • What “physical evidence” are you providing to give tangibility to your program?
Does the program strategy fit with consumer needs? • Price • What is the cost to individuals/agencies? • What do they have to give up? (Time, money, discomfort, effort) • Place • Is where you are delivering the program consistent with needs and accessible? • Go to where people are • People/health professionals will not go looking for your program or message.
Does the program strategy fit with consumer needs? • Processes • Do you have clear referral pathways with multiple entry points? • Does your pathway build on systems in place to embed program? • Intake systems / central coordination / recall and reminder • Do you have strategies to combat obstacles? • Brainstorm and do risk analysis • Walk through the process as a consumer
Does the program strategy fit with consumer needs? • Promotion • Do you have a comprehensive communication program using all types of media? • What is the message you seek to promote? • May have different messages for different target groups • Focus on benefits • Focus on one core proposition e.g. call to action for service providers • Desirable, exclusive and believable
Consumer behaviour • Consumers of a service want information before recruitment • Consumers will prefer personal over impersonal sources of information • Consumers give greater credibility to independent sources of information • Consumer who have had a prior experience with the service are more likely to turn to their memories first before collecting new external information
An example: Communicating risk • Factors influencing thinking on risk • People underestimate risk related to chronic disease overestimate communicable disease • Trust • Who is telling me are they trustworthy? • Risk less acceptable if: • Imposed • Distributed unevenly • Resulting from man made • Hidden/irreversible
An example: Communicating risk • May need to work on changing perception of risk in the community • Set the agenda • Getting the issue on the air • Facilitating the acceptance of change • Promote response efficacy -convince HPs and consumers changing will have an effect • Build self efficacy (consumers and HPs)
Consumer Characteristics & Behaviour Program Strategy • Point of contact • Systems generation referral letters and service coordination tools • Displays • Internet, telephone hold Communication strategy
Know what works and milk it!! • Utilise consumers to test concepts • Continually evaluate • Build referral / recruitment information into practices • Make strategy fluid and change if not working
Key messages • Talk to your target group • Develop and test a definitive plan • Segment your market • Position your program • Know your competition • Go to where your audience is with a program they want • Use a variety of approaches • Use models and systems in place • Build partnerships • Evaluate and rethink
An example – Pre diabetes self management program • Target groups • Consumers with IGT/IFG and/or cardiac disease, obesity, hyperlipidaemia, hypertension etc and past history of GDM in catchment • Key initial key target – people with diabetes in their families • Consumer participation through CHC reference group and diabetes support group with individual interviews of people with IGT/IFG • Service providers • Service providers acute and community • General practitioners, diabetes physicians and educators • Interviewed for needs and processes
An example – Pre diabetes self management program • Program • Evolve program from validated, established diabetes self management program – 4 weeks • Run health professional and consumer team • Physical evidence of information on recruitment flyers and handouts each week of program • Add education about pre diabetes with service providers • Price • $10 cost to consumers for handouts and refreshments • Place • Run over catchment. Initially at CHC then accessible locations eg council offices, acute care, RSL
An example – Pre diabetes self management program • Processes • Referral pathway with multiple intake points from direct referral, service providers, GPs, non health providers (eg community information service) • GP, acute and specialist referral for newly diagnosed with referral pads, electronic referral and practice nurse reminders linked to SC tools • Focus on intake workers/GPs in local settings with electronic tagging and recall and reminder system • Feedback loops to GPs and service providers with consumers permission
Communication strategy - GPs • Point of contact • General awareness, , facilitate referral, reminder • Service coordination tools • Information pack and facilitated help • Electronic reminders, referral pads, posters and ed material in waiting room
Communication strategy - Consumers • Point of contact • Awareness and Reminder of program • Posters and flyers @ service providers • Enrolment information, reminder call and follow-up once enrolled