Download
1 / 33
1.5k likes | 6.51k Views
Assessment of Thorax and Lungs. Christine M. Wilson Viterbo University. Objectives. Landmarks Structures Function Developmental/transcultural Subjective data Objective data. Anterior Landmarks. Clavicle Suprasternal notch Sternum Sternal angle Intercostal spaces Xiphod process

E N D
Assessment of Thorax and Lungs Christine M. Wilson Viterbo University
Objectives • Landmarks • Structures • Function • Developmental/transcultural • Subjective data • Objective data
Anterior Landmarks • Clavicle • Suprasternal notch • Sternum • Sternal angle • Intercostal spaces • Xiphod process • Costal angle
Posterior Landmarks • Vertebra prominens (C7) • Spinous processes • Scapula
Reference Lines Anterior Chest • Midsternal • Midclavicular
Reference Lines Posterior Wall • Vertebral Line • Scapular Line
Reference Lines Axillary Area • Midaxillary • Anterior Axillary • Posterior Axillary
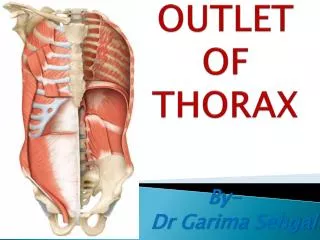
Position in Chest • Lobes of the lung • Trachea • Bronchial Tree
Functions of Respiration Major Functions • Supply oxygen to body for energy production • Remove carbon dioxide as a waste from energy production • Maintain pH balance of arterial blood • Maintain heat exchange
Developmental Considerations Fetal Life • At 5 weeks primitive lung buds emerge • By 16 weeks there are the same # of conducting airways as in the adult. • At 32 weeks surfactant sufficient to sustain life • At birth 70 million primitive alveoli kick in
Developmental Considerations The Aging Adult • Lungs more rigid; harder to inflate • Less surface available for gas exchange • Common increase in AP diameter • Kyphosis: Front to back curvature spine • May fatigue more easily
Transcultural Considerations • Largest chests (descending order): whites, blacks, Asians, Native Americans • Fetal lung maturity reached earlier in black population • Incidence of TB is higher in Asian Americans
Subjective Data • Cough • Shortness of breath • Chest pain with breathing • History of respiratory infections • Smoking history • Environmental exposure • Self care behavior
Objective Data-Posterior Chest Inspect • Shape and configuration • A/P diameter should be less than transverse by 1:2 • Position • Skin color and condition
Posterior Chest Symmetric chest expansion • Place hands at T9-T10 • Equal movement of thumbs with inhaling
Posterior Chest Tactile fremitus • Place ulnar edge on skin; client repeats 99 • Symmetry is expected • Decreases if sound transmission is obstructed Palpate chest wall
Posterior Chest Percussion • Find predominant note over lung fields • Begin at apices • Use same pathway side to side
Lung Percussion Sounds • Resonance: non-musical; healthy lung • Hyper-resonance: slightly musical; too much air, i.e. emphysema/pneumothorax • Dull: muffled; organ or abnormal density, i.e. pneumonia • Flat: soft thud; i.e. muscle mass, bone
Posterior Chest Diaphragmatic Excursion • Find lower lung border in expiration and inspiration • Measure: Should measure 3-5cm, equal distance bilaterally.
Posterior Chest Auscultation • Use diaphragm of stethoscope; place firmly • One full breath at each position • Use same pathway • side to side comparison
Breath Sounds • Bronchial • Loud, harsh sounds over trachea • Bronchovesicular • Moderate, mixed sounds over bronchi • Vesicular • Soft, rustling sounds over periphery
Decreased or Absent Obstruction • Secretions, mucus plug, foreign body Emphysema • Loss of elasticity; air already in lungs Silent chest • No air is moving in or out of lungs; ominous sign
Increased Sounds Bronchial sounds heard over wrong area • Solid tissue conducts sounds to surface better • Found in pneumonia with consolidation or fluid in intra-pleural space
Adventitious Sounds Crackles (Rales): Fine • Fine, discontinuous high-pitched, short crackling sound on inspiration which are not cleared by coughing. (Roll a strand of hair at ear) • Found in pneumonia and heart failure
Adventitious Sounds Crackles: Coarse • Loud, low-pitched bubbling or gurgling sounds • Start in inspiration, may be in expiration • Decrease with coughing, but comes back • Found in pulmonary edema and terminally ill with suppressed cough reflex
Adventitious Sounds Wheeze: High pitch • High-pitched, musical squeaking sound that predominates with expiration • Indicates narrowed passageway • Obstruction from acute asthma or chronic emphysema
Adventitious Sounds Wheeze Low-pitch • Single note which is more prominent on expiration • Air flow obstruction • bronchitis or tumor
Adventitious Sounds Stridor • High-pitched, crowing sound with inspiration • Louder in neck • Upper airway obstruction • Croup, acute epiglottis, or foreign body inhalation
Objective Data-Anterior Chest Inspect • Shape and configuration • Facial expression • Level of consciousness • Color and condition • Respiration rate/quality
Anterior Chest Symmetric chest expansion • Place hands at costal margins • Equal movement of thumbs with inhaling
Anterior Chest Tactile fremitus • Apices to MCL • Side to side • Symmetry expected Palpate chest wall
Objective Data-Anterior Chest Percussion • Dullness over breast tissue, liver, cardiac borders • Tympany over gastric Auscultation • Displace breast and listen over chest wall