Download

1 / 17
170 likes | 363 Views
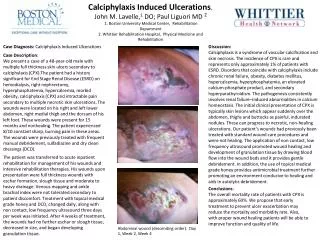
Calciphylaxis AM report Lisa Rose-Jones, MD May 2, 2009. Pathology of “Calcific Uremic Arteriolopathy”. Poorly understood Systemic medial calcification of arteries that lead to ischemia

E N D
Pathology of “Calcific Uremic Arteriolopathy” • Poorly understood • Systemic medial calcification of arteries that lead to ischemia • Histologically see 1)small vessel mural calcification w or w/o fibrosis (absence vasculitic changes) 2) extravascular calcification 3) vascular thrombosis
Calcium deposition. (A) Hematoxylin-and-eosin staining shows calcifications (purple color) in the walls of arterioles and inflammatory changes in the adipose tissue as a result of ischemia. (B) Calcium deposits can be confirmed by von Kossa's staining, which reveals calcium (black color) in the intima of small- and medium-sized arterioles. Demonstrated here is the characteristic circumferential medial calcific deposit in an arteriole with subintimal edema.
Epidemiology • 1st described in rats 1962 • Most commonly affects those w/ Stage 5 CKD who are on HD and those recently who have recv’d renal transplant • Other reported case reports w/ occurrence in Breast Ca, Alcoholic Liver dz, Chron’s, RA, SLE, Primary Hyperparathyroid
Epi continued…… • True incidence not known, believed to affect 1-4% of pts w/ ESRD • Affects Caucasians >> African Americans • 3 Females :1 Male • One study suggested seen in younger patients w/ history of long duration of HD
Why An Association with ESRD • ?Role of PTH – suggested by beneficial effect of parathyroidectomy = transient uptake of Ca,P (hungry bone) and lower Ca XP product • High doses Vit D induces this in animal models, interesting since analogs like Calcitriol administered to tx 2ndary Hyperparathryoidism in ESRD pts
Other triggers? • Long-term obesity • Recent and sudden weight loss • Malnutrition • Infusion of medications such as iron dextran • Remote and/or recent use of immunosuppressive agents, especially corticosteroids • Liver disease • Diabetes mellitus and insulin injections • Use of vitamin D and calcium-based phosphate binders • Concurrent use of warfarin anticoagulation: Current data suggest that warfarin therapy may lower protein C concentrations, leading to a procoagulant condition in the calcified vessel. Warfarin may also inhibit carboxylation of matrix Gla protein, an important inhibitor of calcification, thus promoting calcification
Clinical Manifestations: • From ischemia one then develops livedo reticularis and/or violaceous painful plaque like subcutaneous nodules where there is most abundant adipose (trunk, buttocks, and proximal extremities)
. The patient in Panel A suffers from end-stage renal disease and has been treated with hemodialysis for more than 4 years. She has had ischemic, nonhealing necrotic ulcerations on her calves for more than 4 months. The patient in Panel B, who was on peritoneal dialysis, presented with a 2-month duration of well-demarcated erythema, hemorrhagic bullae, ulcers, and ecchymoses surrounded by skin thickening and tender subcutaneous indurations.
Clinical Manifestations: • Ulceration is considered a late finding and is associated with a higher mortality rate • Multiple lesions of variable age may be present, following the path of the vasculature. • Less commonly, lesions may manifest as either bullae or distinct subcutaneous, erythematous nodules.
Diagnosis: • Plain films reveal vascular calcifications w/in dermis or subQ tissue (non-specific). ?mammography • Bone Scan can reveal abnormal uptake • Deep Incisional Biopsy** risky • Rule out HyperCoag states and Cryoglbulinemia ~There is no threshold of levels for PTH, Ca, or Phos to exclude/estb this diagnosis
Treatment: • Lower Ca x P product to < 55 w/ non-calcium containing Phosphate binders such as Sevelamer or Lanthanum • Cinacalcet (increases Ca receptor sensitivity to Ca thus normalizing PTH secretion) • Bisphosphonates • ? Role of urgent parathryoidectomy
Pain Management is extremely Important • Surgical c/s for wound care & debridement • Hyperbaric Oxygen therapy has proven successful in several cases
Sodium Thiosulfate – a Novel therapy? • A potent antioxidant that increases solubility of calcium deposits • IV use for calciphylaxis is off-label • Generally well tolerated, but must watch for Anion Gap metabolic Acidosis
~Prognosis • Mortality rate as high as 60-80% in pts w/ ulcerative disease • Most patients succumb to sepsis from their wound infections or organ failure from internal involvement (stone heart) • Location of skin lesions helps predict outcomes: those proximal to elbows/knees (63%) vs distal (23%)
References: Uptodate Cicone JS, Petronis JB, Embert CD, Spector D. Successful treatment of calciphylaxis with intravenous sodium thiosulfate. Am J. Kidney Dis. Jun 2004; 43(6)1104-8. Don BR, Chin AI. A strategy for the treatment of calcific uremic arteriolopathy (calciphylaxis) employing a combination of therapies. Clin Nephrol. 2003;59:463-470. Weenig RH, Sewell LD, Davis MD, et al. Calciphylaxis: natural history, risk factor analysis, and outcome. J Am Acad Dermatol. 2007;56:569-579.