Download
1 / 54
690 likes | 1.25k Views
THE COMPLEMENT SYSTEM. Sections from chapter 2 and 11 in Parham’s book . Complement system.

E N D
THE COMPLEMENT SYSTEM Sections from chapter 2 and 11 in Parham’s book
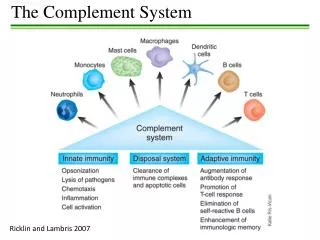
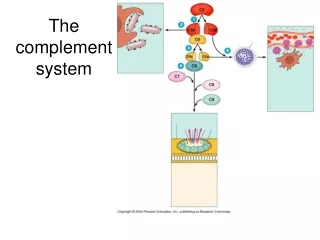
Complement system The complement system is a set of about 30soluble proteins, constitutively produced by the liver, that are found in the blood, lymph and extracellular fluids,and act against extracellular pathogens. Complement activation proceeds by a cascade of enzymatic reactions (proteases), in which each protease cleaves and activates the next enzyme in the pathway.
C3 CGEQ One of the proteins present at the highest concentration in serum 1.2mg/ml THE CENTRAL COMPONENT OF THE COMPLEMENT SYSTEM CLEAVAGE SITE (3900000000000000 molecules/ml)
C3 CGEQ CGEQ R R O O CGEQ CGEQ R R R R R OH OH OH OH OH C3a C3b Cell Binding Inflammation Bacterium
Complement fixation- Covalent binding of C3b to the pathogens’ surface
The alternative pathway The alternative soluble C3 convertase
AMPLIFICATION OF THE COMPLEMENT CASCADE inactive precursors limited proteolysis enzyme activating surface
Regulation of the complement system Positive regulation Negative regulation (Inhibits both alternative and classical convertases)
DAF and MCP Negative regulatory proteins on human cells protecting them from complement-mediated attack MCP binds to sialic acid on the surface of human cells and prevents the complement activation
Eukariotic cells GLYCOSYLATION OF PROTEINS IS DIFFERENT IN VARIOUS SPECIES Prokariotic cells Sialic acid Galactose Glucoseamine Neuraminic acid (Sialic acid) Mannose
The classical pathway THE C1 COMPLEX C1qR binding by Phagocytes Cleavage of C4 and C2 components Collagen „legs” Gobular „heads” Binding the Fc part of an antibody
Immunoglobulin Fragments: Structure/Function Relationships antigenbinding complement binding site binding to Fc receptors placental transfer C1 component ‘heads’ Association between native and adaptive immunity Only the antigen-linked antibodies are able to associate to complement.
Low affinity binding to the C-terminal of an antibody Multiple interactions with immune complexes
CRP binds to phosphocholine component of the lipopolisaccharides in bacterial and fungal cell wall but not to phosphocholine component of phospholipids on human cell membranes!
ACUTE-PHASE RESPONSE INCREASES THE SUPPLY OF INNATE IMMUNITY MOLECULES C-reactive protein CRP levels can increase up to 1000-fold during an acute-phase response!
One of the major function of C1 INHIBITOR C1q binds to IgM on bacterial surface C1q binds to at least two IgG molecules on bacterial surface Binding of C1q to Ig activates C1r, which cleaves and activates the serine protease C1s C1INH dissociates C1r and C1s from the active C1 complex
The Mannose-binding Lectin pathway • Binds Mannose-containing carbohydrates of bacteria, fungi, protozoans and viruses • Similar to C1q protein in triggering a complement cascade • MASP-1 and 2 have common gene ancestors with C1r and C1s • A member of the Collectin family
Eukariotic cells Mannose GLYCOSYLATION OF PROTEINS IS DIFFERENT IN VARIOUS SPECIES Prokariotic cells Galactose Glucoseamine Neuraminic acid (sialic acid) Mannose
ACUTE-PHASE RESPONSE INCREASES THE SUPPLY OF INNATE IMMUNITY MOLECULES Mannose-binding lectin MBL levels can increase up to 1000-fold during an acute-phase response! * SP-A and SP-D belong to the collectin family as well, opsonyzing pathogens in the lung
Local inflammatory responses can be induced by the small complement fragments C3a, C4a, and especially C5a
Bacterium complement receptors macrophage Opsonization C3b Ex:CR1, CR3, CR4
Membrane attack complex (MAC) C3bBbC3b = alternative C5 convertase Or C4bC2aC3 = classical C5 convertase
The membrane-attack complex assembles to generate a pore in the lipid bilayer membrane
CD59 prevents assembly of terminal complement components into a membrane pore
Immune complex diseases • Early components of the classical pathway (C1-C4) are necessary for the elimination of immune complexes! Attachment of the complement components to the soluble immune complexes allows them to be transported, or ingested and degraded by CR-bearing cells. • Deficiencies in these components lead to the accumulation of immune complexes in the blood, lymph and extracellular fluid and their deposition in tissues. Damage is caused by the deposition itself and by the activation of phagocytes causing inflammation. • These may include: • Pyogenic infections • Systemic Lupus Erythematosus • Vasculitis • Glomerulonephritis
Paroxysmal Nocturnal Hemoglobinuria (PNH) Acqired clonal mutation of PIG-A gene no GPIenchor proteins on RBCs No expression of the complement regulatory proteins CD59 and DAFon these RBCs episodes of complement-mediated RBCs lysis hemolytic anemia Symptoms include: Anemia (tiredness, shortness of breath, palpitations) Hemoglobin in the urine 40% develope thrombosis Therapy include: Anti-C5-Mab, transfusion, immunosuppression and BM transplantation.
Hereditary Angioneuretic Adema (HANE) Deficiency in C1INH complement regulatory protein. The C1INH is a serine protease inhibitor that regulates the C1 complex and complement activation as well as inhibiting proteins in the coagulation cascade. Symptoms include: swellings of skin, gut and respiratory tracts serious acute abdomenal pain, vomiting Therapy include: C1INH from donor blood, Androgens and other bradykinin inactivators
Major regulating factors of complement system C1Inh: C1-inhibitor (serine-protease inhibitor, can affect in many steps) Factor H: inhibits C3-convertase of alternative pathway, co-factor of factor I, cleaves C4b and C3b Properdin: stabilizes convertases of alternative pathway DAF: Decay Accelerating Factor MCP: Membrane Cofactor Protein CD59: inhibits the linking of C9 and C8
Factor I DAF C1Inh C4bp CR1 MCP HRF C-pept.ase N CD59 S-protein DAF Fact-H CR1 MCP Factor I positive feedback Regulation of complement system a-2macrogl LECTIN PATHWAY Properdin membrane protein soluble molecule
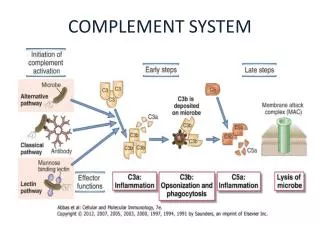
COMPLEMENT SYSTEM CLASSICAL PATHWAY MB-LECTIN PATHWAY ALTERNATIVE PATHWAY Antigen-antibody complex Mannose Pathogen surface MBL MASP-1/MASP-2 Serin protease C4, C2 C3 B, D C1q, C1r, C1s Serin protease C4, C2 C4a* C3a, C5a C3 CONVERTASE C3b Terminal C5b – C9 Inflammatory peptid mediators Phagocyte recruitment Opsonization Binding to phagocyte CR Immune complex removal MAC Pathogen/cell lysis
Deficiencies of complement system – regulatory molecules, receptors
Hereditary angioneurotic edema (HANE) (hereditary C1INH defect) • 17-year old boy - severe abdominal pain (frequent sharp spasms, vomiting) • appendectomia normal appendix • similar symptoms occured repeatedly earlier in his life with watery diarrhea • family history of prior illness • immunologist’s suspicion: hereditary angioneurotic edema • level of C1INH: 16% of the normal mean • daily doses of Winstrol (stanozolol) – marked diminution in the frequency and • severity of symptoms • purified C1INH intravenously became avaible by the time • Main symptoms: • swellings of skin, guts, respiratory tracts • serious acute abdomenal pain, vomiting • larynx swelling – may cause death • Treatment: • iv C1INH • kallikrein and bradykinin receptor antagonists Child with symptomes of HANE
Pathogenesis of hereditary angioneurotic edema Inhibition by C1INH in many steps activation of XII factor • bradykinin and C2-kinin: • enhance the permeability of • postcapillar venules • by contraction of endothel • holes in the venule walls • edema formation • C1 is always active without • activating surface because • plasmine is always active activation of kallikrein activation of proactivator cleveage of kininogen to generate bradykinin, vasoactive peptide cleveage of C2a to generate C2-kinin, vasoactive peptide cleveage of plasminogen to generate plasmin cleveage of C2 to generate C2a activation of C1