Download
1 / 46
460 likes | 491 Views
This introduction to cancer genetics covers the types of cancer syndromes, genetic testing, and counseling services available. It explains the population cancer risks and the difference between sporadic, familial, and hereditary cancers. The text outlines the aims of genetic counseling and the referral guidelines for assessing cancer risk, along with tools such as the Manchester score and BOADICEA algorithm. It also discusses genetic testing for hereditary cancer, the implications of carrying cancer susceptibility genes, and the options available for individuals with a higher risk, such as surgery and surveillance. Specific focus is placed on hereditary breast and ovarian cancers caused by BRCA1/2 mutations, including lifetime risks and management options. The significance of genetic testing, implications for cancer development, and surveillance recommendations are highlighted for individuals with hereditary cancer predispositions.

E N D
Introduction to Cancer Genetics Emma Williams Genetic Counsellor NE Thames Regional Genetics Service
Overview Cancer Syndromes & Management options Genes & Genetic testing Genetic Counselling & Cancer Genetic Service Population cancer risk
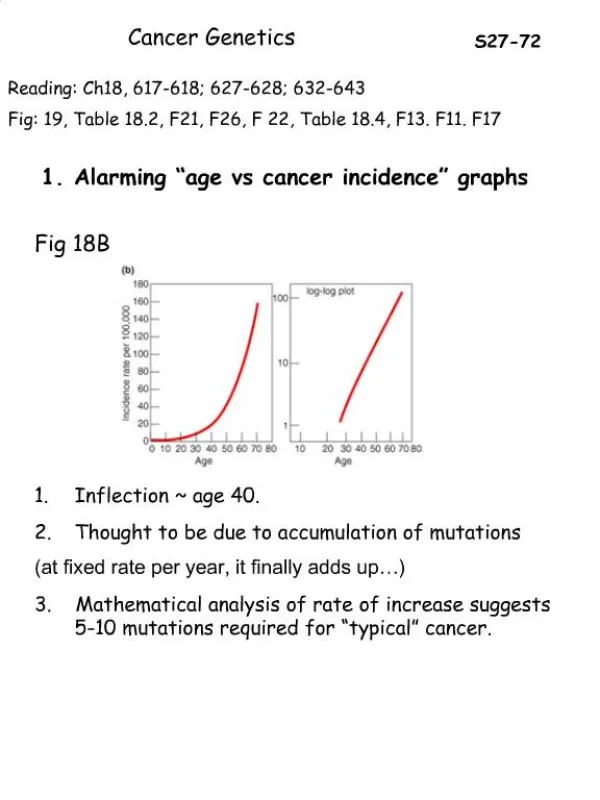
What are the cancer risks for the general population? • 1 in 3 people will develop cancer at some point in their lives • Prostate: 17% • Female Breast: 12-13% • Lung: 6-8% • Colorectal cancer: 6% • Melanoma: 1-2% • Ovarian: 1.5% • Stomach / Pancreas: 1% • Male breast: 0.1% SEER Figures. NCI 2001-2003
How Many Cancers are Genetic? Sporadic (~85%) Familial (~10%) Hereditary (~5%)
Many patients may have a similar FHx Age of diagnosis typically later in life Usually not inherited Can be reassuring Sporadic Cancer
Aims of Genetic Counselling Help patients to… • Understand the information about the genetic condition • Appreciate inheritance patterns and risk of recurrence • Understand available options • Make informed choices appropriate to their personal and family situation • Make the best possible adjustment to the condition and risk
Referral guidelines http://www.ich.ucl.ac.uk/gosh/clinicalservices/Clinical_genetics/Custom%20Menu_01
Risk Assessment Tools • Referral guidelines / NICE guidelines • Family History form • Comprehensive 3 generation pedigree • Confirmation of cancer pathology • Pedigree assessment • Manchester score • BOADICEA (Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm) • Amsterdam I/II Criteria • Bethesda Criteria
Genetic Cancers • Breast and ovarian • Colon cancers • Cowden syndrome • Gastric cancer • Gorlin Syndrome • Li-Fraumeni • Multiple endocrine neoplasia (MEN) • Neurofibromatosis • Peutz-Jeghers syndrome • Phaeochromocytoma • Retinoblastoma • von Hippel-Lindau disease • Wilm’s tumour
Several affected family members Earlier than average age of onset Multiple generations are affected on one side of the family A particular pattern of cancers noted Individuals with more than one primary tumour site 5-10% of Cancer Cases Hereditary Cancer
Most Cancer Susceptibility Genes Are Dominant With Incomplete Penetrance • You only need one altered copy of the gene to have an increased risk of cancer • Gender is irrelevant • It is not possible to “skip” generations • Penetrance can be incomplete • All offspring are at 50:50 risk Normal Susceptible Carrier Carrier, affected Ca Sporadic Ca
Genetic Testing • Genetic testing is usually carried out on DNA from a blood sample • Technically difficult to locate the mutation in a cancer gene for a particular family • Can take up to three months • Usually need to first test a living relative who has already developed cancer • Is only offered to high risk families (>20% chance of mutation) • Often cannot locate a mutation in a family (only identified in about 20% of families)
Genetic Testing cont… • Genetic testing is NOT usually possible if there are no living affected relatives • Exception is populations with founder mutations eg Ashkenazi Jewish population • Once a mutation is found, testing can be offered to other at-risk family members • Individuals who DO NOT carry the family mutation ARE NOT at increased risk of developing the cancers, but are still at population risk • Individuals who DO carry the family mutation ARE at increased risk of developing cancer but there is still uncertainty. . . However, testing enables us to identify individuals who may be at higher risk of developing certain types of cancer
Accounts for 4-5% breast cancer cases 40-70% lifetime risk breast cancer 10-45% lifetime risk ovarian cancer Increased risk prostate cancer in male carriers Genetic testing possible for some families Surgery and surveillance options for affected individuals Hereditary Breast and Ovarian Cancer Other genes • Most cases caused by a mutation in BRCA1 or BRCA2 gene • BRCA1 / 2 are tumour suppressor genes, which are involved in the repair of DNA • Accounts for about 5% of breast cancer cases and about 12% of ovarian cancer cases BRCA1 BRCA2 5-10% Sporadic Hereditary
BRCA1 -Associated Cancers: Lifetime Risk Breast cancer 56%-87% (often early age at onset) Second primary breast cancer 64% Ovarian cancer 16%-44% Increased risk of other cancers, eg about double population risk for prostate cancer in men
BRCA2-Associated Cancers: Lifetime Risk breast cancer (50%-80%) male breast cancer (7%) contralateral breast (50%) prostate (~30%) ovarian cancer (15-27%) Other cancers: pancreatic malignant melanoma
Options for BRCA1/2 Carriers Cancer Screening Additional breast screening by mammography / MRI Ovarian screening through UKFOCSS research trial Prophylactic bilateral mastectomy ~90% reduction in breast CA risk Prophylactic bilateral salpingo-oophorectomy ~up to 96-98% reduction in ovarian CA risk ~50% reduction in breast CA risk (age dependant) ? Chemoprevention in the future ? Tailoring of treatment for carriers in the future
When to refer • 2 first or second degree relatives with breast cancer < 50 yr • 3 first or second degree relatives with breast cancer <60yr • 4 relatives with breast cancer at any age • 1 ovarian cancer at any age + 1 breast cancer < 50yr • 1 ovarian cancer + 2 breast cancer both < 60y • 2 ovarian cancer any age • Patients who are thought to be of Ashkenazi Jewish heritage with at least one first degree relative with breast cancer <50 years or ovarian cancer any age • NB bilateral breast primaries equivalent to 2 relatives
HNPCC or Lynch syndrome Hereditary non-polyposis colorectal cancer (HNPCC) • 3-5% of all colorectal cancer cases • Autosomal dominant – multiple generations affected • High penetrance • Typical age of CA onset is 40-50 yrs • 60-70% right-sided/proximal CRC tumors • Polyps may be present, multiple primaries common. Can overlap with AFAP
HNPCC • Lifetime cancer risks: • Colorectal 80% • Endometrial 20-60% • Gastric 13-19% • Ovarian 9-12% • Biliary tract 2% • Urinary tract 4% • Small bowel 1-4% • Brain/CNS 1-3%
HNPCC Caused by mutations or deletions in mismatch repair (MMR) genes MMR genes are like spell checkers in our DNA. • MSH2, MLH1, MSH6, PMS2 • 90% of detectable mutations in MSH2 and MLH1 • 7-10% of detectable mutations in MSH6
Options for individuals withHNPCC • 1-2 yearly colonoscopy • Ovarian and endometrial screening (not proven to be effective) • ? renal/upper GI screening effective (if have history of gastric/renal cancers) • Surgery • Prophylactic bowel surgery not often chosen • Total abdominal hysterectomy and salphingo oophorectomy for females
Familial adenomatous polyposis (FAP) • 1 in 10,000 incidence • 100’s to 1000’s of colonic adenomas by teens • 7% risk of CRC by 21 yrs; 93% by 50 yrs • 20-25% no history in parents • Extra-colonic features • Screening • 1 – 2 yearly flexible sigmoidoscopy from age 10 – 12 • Upper GI endoscopy 1 –3 yearly from age 25
MAP syndrome/MYH gene • MYH associated Polyposis (MAP) syndrome • Autosomal recessive; mutations in the MYH gene • Median number of polyps = 55 • Mean age of polyp diagnosis = 30-50 years • Polyps mainly small, mildly dysplastic tubular adenomas. Some tubulovillous, hyperplastic, serrated adenomas, microadenomas • 30% of individuals with 15-100 polyps have homozygous mutations in the MYH gene • Genetic testing should be offered if >10-15 polyps (and APC gene testing negative)
When to refer • Patient or 1 first degree relative affected with • Colorectal cancer <50yrs • 2 or more colorectal primary cancers any age • Colorectal cancer and a related cancer* any age. • 2 first degree relatives affected with colorectal cancer or related cancer* at any age • 3relatives affected with colorectal cancer or related cancer* at any age, one of which must be a first degree relative. • History of Polyposis (e.g. Familial adenomatous Polyposis) • *related cancers- endometrial, ovarian, small bowel, ureter, renal pelvis and stomach
Genetics and Uncertainty • Cancer genetics is not relevant for most people • Cancer genetics is not a crystal ball • But cancer genetics can have a great impact on those families most at risk of familial cancer
What Can You Do? • Recognise patterns of cancers in families • Young onset • Lots of one or two particular types of cancer • Jewish? • If not sure ask • Don’t be afraid to contact genetics for advice • Take a blood sample for DNA banking
DNA Banking • DNA banking provides families with the chance to pursue genetic testing at a later point in time. • where there is currently no genetic test available. DNA banking will allow the family to take advantage of future advances in genetic testing technology. • A family member diagnosed with cancer who is terminally ill and there is no time for traditional a genetic assessment and/or testing. The family can then focus their attention on their loved one and defer the process of genetic counselling and testing to a time when they are ready.
Contact Details Emma Williams Registered Genetic Counsellor NE Thames Regional Genetics Service Great Ormond Street Hospital Great Ormond Street London, WC1N 3JH email: emma.williams@gosh.nhs.uk Tel: 0207 905 2625 Fax: 0207 813 8141
Case 1: Ruth Ruth, a 35 year old Ashkenazi Jewish woman, comes because she is anxious about her family history of cancer. You inquire about family health history and find out the following information: Paternal family history is as follows: Paternal grandmother diagnosed with ovarian cancer age at 63 Paternal aunt diagnosed with breast cancer age 42 Ruth has no other risk factorsor pertinent family history
Case 1: Pedigree Polish Jewish Russian Jewish Dx 63 82 yrs 60 58 Dx 42 64yrs Key -Ov Ca Ruth 35 38 41 -Br CA
Case 1: Assessment Patient is in “Moderate risk” category However ethnicity is important as she is of Ashkenazi Jewish descent Refer to genetics clinic Moderate risk screening for breast cancer arranged Genetic testing for 3 common ‘Jewish Mutations’
Case 2: Ann Ann has come along because her sister has ovarian cancer, sadly the cancer has spread. Her family history is a follows: Sister diagnosed with ovarian CA at 53 yrs. Mother diagnosed with ovarian CA at 61 yrs and has sadly died. Maternal aunt diagnosed with breast cancer at 48 yrs. Ann has no other risk factors for breast cancer. She feels that with her family history, cancer is inevitable
Case 2: Pedigree Dx 61 Died 64 Dx 48 73 65 3 39 30s DX 53 49 2 2
Case 2: Assessment Patient is in “High” risk category Refer to genetics clinic promptly High risk screening breast and ovarian cancer Genetic testing offered
Case 3 • Helen has primary ovarian cancer • Would this family need seeing by genetics? • What other cancer could she be at risk for? YES Colon and uterine cancers
Case 4 French, Irish, Scottish German, English 88 yr Dx 50 61 yr 63 yr CRC Dx 48 4 polyps 50 yrs. Key: 38 yr 35 yr Endometrial CA Dx 38 Colorectal CA Adenomatous polyps Lynch syndrome 8 yr 10 yr
Case 5 • Would you refer this gentleman to genetics? • What else would you ask about the family? YES Is he Jewish? He has a BRCA mutation!
Case 6 • Which side of the family are you worried about? • What surveillance does she need? Both Breast and ovarian screening She actually had two BRCA mutations!
Case 7: Ted • Ted is 30 and wants a colonoscopy because his mother was just diagnosed with colon cancer after routine screening at age 54. Family history reveals: • Paternal grandfather: died of CRC at age 79. • No hx of endometrial, ovarian, small bowel or ureter/kidney cancer on either side of family. • Two maternal aunts: cervical cancer at ages 30 & 34 • Maternal grandmother: breast cancer age 85 Reassure
Case 8: Alison Alison is a 40 year old Caucasian (non-Jewish) patient who asks you for information about the “breast cancer gene test”. She states she wants this test. You ask about her family history: Mother with breast cancer - age 58 Maternal aunt with breast cancer – age 65 Paternal grandmother with breast cancer – age 79 Alison has no other risk factors for breast cancer She feels that with her family history, breast cancer is inevitable
Case 8: Pedigree British German/Dutch Dx 79 d.81 Dx 58 65 yr Dx 65 71 yr Key: -Breast CA Alison 40 yr 15 yr
Case 8: Assessment Patient is in “Moderate” risk category Refer to breast clinic for breast cancer screening from 40-50 years then NBSP Counselling issues: Unlikely to be due to a BRCA1 or BRCA2 mutation Screening and preventive strategies Psychosocial – perceived risk, fears Support resources