Download
1 / 1
30 likes | 270 Views
Bed rest versus ambulation in the initial treatment of patients with proximal deep vein thrombosis. SUMMARY. Treatment for DVTs include low molecular weight heparin (LMWH) and oral anticoagulants In the past, physicians have recommended 4 to 5 days of bed rest for patients with a DVT

E N D
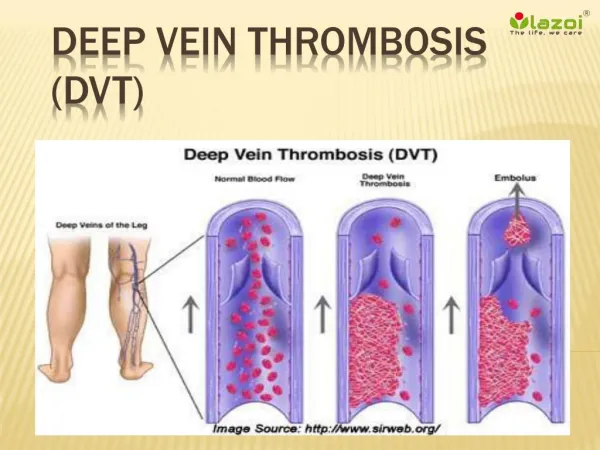
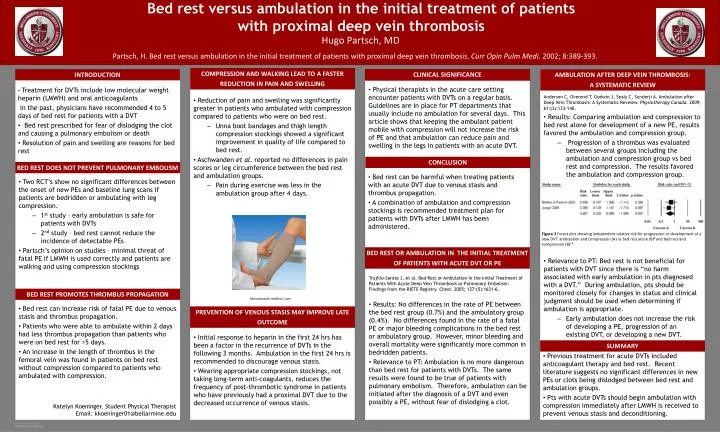
Bed rest versus ambulation in the initial treatment of patientswith proximal deep vein thrombosis SUMMARY Treatment for DVTs include low molecular weight heparin (LMWH) and oral anticoagulants In the past, physicians have recommended 4 to 5 days of bed rest for patients with a DVT Bed rest prescribed for fear of dislodging the clot and causing a pulmonary embolism or death Resolution of pain and swelling are reasons for bed rest INTRODUCTION Hugo Partsch, MD Partsch, H. Bed rest versus ambulation in the initial treatment of patients with proximal deep vein thrombosis. CurrOpinPulmMedi. 2002; 8:389-393. BED REST DOES NOT PREVENT PULMONARY EMBOLISM Reduction of pain and swelling was significantly greater in patients who ambulated with compression compared to patients who were on bed rest. • Unna boot bandages and thigh length compression stockings showed a significant improvement in quality of life compared to bed rest. Aschwandenet al. reported no differences in pain scores or leg circumference between the bed rest and ambulation groups. • Pain during exercise was less in the ambulation group after 4 days. COMPRESSION AND WALKING LEAD TO A FASTER REDUCTION IN PAIN AND SWELLING AMBULATION AFTER DEEP VEIN THROMBOSIS: A SYSTEMATIC REVIEW Anderson C, Overend T, Godwin J, Sealy C, Sunderji A. Ambulation after Deep Vein Thrombosis: A Systematic Reveiew. Physiotherapy Canada. 2009; 61:(3):133-140. Results: Comparing ambulation and compression to bed rest alone for development of a new PE, results favored the ambulation and compression group. • Progression of a thrombus was evaluated between several groups including the ambulation and compression group vsbed rest and compression. The results favored the ambulation and compression group. Relevance to PT: Bed rest is not beneficial for patients with DVT since there is “no harm associated with early ambulation in pts diagnosed with a DVT.” During ambulation, pts should be monitored closely for changes in status and clinical judgment should be used when determining if ambulation is appropriate. • Early ambulation does not increase the risk of developing a PE, progression of an existing DVT, or developing a new DVT. BED REST OR AMBULATION IN THE INITIAL TREATMENT OF PATIENTS WITH ACUTE DVT OR PE Trujillo-Santos J, et al. Bed Rest or Ambulation in the Initial Treatment of Patients With Acute Deep Vein Thrombosis or Pulmonary Embolism: Findings from the RIETE Registry. Chest. 2005; 127:(5):1631-6. Results: No differences in the rate of PE between the bed rest group (0.7%) and the ambulatory group (0.4%). No differences found in the rate of a fatal PE or major bleeding complications in the bed rest or ambulatory group. However, minor bleeding and overall mortality were significantly more common in bedridden patients. Relevance to PT: Ambulation is no more dangerous than bed rest for patients with DVTs. The same results were found to be true of patients with pulmonary embolism. Therefore, ambulation can be initiated after the diagnosis of a DVT and even possibly a PE, without fear of dislodging a clot. CLINICAL SIGNIFICANCE Two RCT’s show no significant differences between the onset of new PEs and baseline lung scans if patients are bedridden or ambulating with leg compression. • 1st study – early ambulation is safe for patients with DVTs • 2nd study – bed rest cannot reduce the incidence of detectable PEs Partsch’s opinion on studies – minimal threat of fatal PE if LMWH is used correctly and patients are walking and using compression stockings Physical therapists in the acute care setting encounter patients with DVTs on a regular basis. Guidelines are in place for PT departments that usually include no ambulation for several days. This article shows that keeping the ambulant patient mobile with compression will not increase the risk of PE and that ambulation can reduce pain and swelling in the legs in patients with an acute DVT. Katelyn Koeninger, Student Physical Therapist Email: kkoeninger01@bellarmine.edu Bed rest can increase risk of fatal PE due to venous stasis and thrombus propagation. Patients who were able to ambulate within 2 days had less thrombus propagation than patients who were on bed rest for >5 days. An increase in the length of thrombus in the femoral vein was found in patients on bed rest without compression compared to patients who ambulated with compression. Bed rest can be harmful when treating patients with an acute DVT due to venous stasis and thrombus propagation. A combination of ambulation and compression stockings is recommended treatment plan for patients with DVTs after LMWH has been administered. Initial response to heparin in the first 24 hrs has been a factor in the recurrence of DVTs in the following 3 months. Ambulation in the first 24 hrs is recommended to discourage venous stasis. Wearing appropriate compression stockings, not taking long-term anti-coagulants, reduces the frequency of post-thrombotic syndrome in patients who have previously had a proximal DVT due to the decreased occurrence of venous stasis. CLINICAL SIGNIFICANCE BED REST PROMOTES THROMBUS PROPAGATION CONCLUSION PREVENTION OF VENOUS STASIS MAY IMPROVE LATE OUTCOME Previous treatment for acute DVTs included anticoagulant therapy and bed rest. Recent literature suggests no significant differences in new PEs or clots being dislodged between bed rest and ambulation groups. Pts with acute DVTs should begin ambulation with compression immediately after LMWH is received to prevent venous stasis and deconditioning. Figure 3 Forest plot showing independent relative risk for progression or development of a new DVT: ambulation and compression (A) vs bed rest alone (B)6 and bed rest and compression (B)19. Mountanside-medical .com