Download
1 / 15
270 likes | 1.61k Views
Hereditary Macular dystrophies. Optometry 8370 Spring 2008. Stargardt Disease. Introduction Most common inherited macular dystrophy 8,000-10,000 Americans Abnormal lipofuscin disease of the RPE Non-progressive. Stargardt Disease. Introduction Usually young age of onset (teen)

E N D
Hereditary Macular dystrophies Optometry 8370 Spring 2008
Stargardt Disease • Introduction • Most common inherited macular dystrophy • 8,000-10,000 Americans • Abnormal lipofuscin disease of the RPE • Non-progressive
Stargardt Disease • Introduction • Usually young age of onset (teen) • Typically autosomal recessive • Mutation on ABCA4 gene (chomosome #1) • Genetic testing available
Stargardt Disease • Introduction: terminology • Fundus flavimaculatus • Bilateral and progressive, flecks • Stargardt Disease • Juvenile macular dystrophy • Risk of CNV
Stargardt Disease • Pathology • Gene mutation • Buildup of fluorophore A2E • Buildup of lipofuscin • Photoreceptor cell death
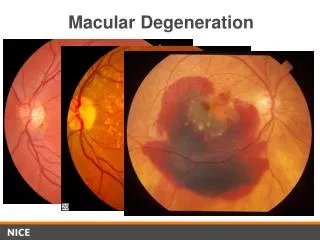
Stargardt Disease • Typical patient • Myopic teen with gradual vision loss • Signs • Macular granularity beaten bronze or metallic appearance (“Bull’s eye”) • Deep yellowish pisciform or “fishtail” retinal flecks made of lipofuscin ; posterior pole and may spread outward • Variability of signs…one without the other • OU
STARGARDT DISEASE • Course of VA • Probability of maintaining 20/40 VA in one eye • By age 19, > 50% • By age 29, > 30% • By age 39, > 20%
Stargardt Disease • Diagnosis • Fundus appearance • Normal ERG • Fluorescein Angiography to confirm • Macular window defects • Darkened choroidal flush
STARGARDT DISEASE • Management • No current medical treatment available • Future: drug to prevent A2E buildup • Low vision aids if needed • Counseling: genetic and psychological
Best VITELLIFOrm dystrophy • Introduction • Macular accumulation of lipofuscin disorder • Autosomal dominant • Defective genes: VMD2 (chromosome #11) and RDS (chromosome) • Ecode for Bestrophin protein and perpherin, which aid with photoreceptor function
BEST Vitteliform dystrophy • Introduction • Diffuse effects on RPE • Early and adult-onset forms • Lesion at < 10 years • About 75% of patients < 40 have BVA of 20/40 in at least one eye
BEST ViTELLIFORM DYSTROPHY • Typical patient • Signs • Initial circular macular lesion (egg yolk) • OU, may be asymmetric • Asymptomatic (slight decrease in VA) because lesion subretinal • ½ -5 DD in size • With progression, lesion breaks up (scrambled egg) • Breaks in Bruchs and disruption of overlying sensory retina • Possible CNV with decreased VA and metamorphopsia
Best Vitteliform dystrophy • Diagnosis • Fundus appearance • EOG (Electro-oculogram) • Measures electrical potential generated by RPE/photoreceptor complex • Tests RPE function, will be abnormal • Especially good if fundus signs minimal • Fluorescein angiography for CNV suspect • OCT? • Genetic testing to confirm VMD2 mutations: $150
BEST Vitteliform dystrophy • Diagnosis: EOG • Test generates light and dark amplitudes • Arden ratio: ratio of the amplitudes (light:dark) • Normal 2:1 • Abnormal< 1.6:1 • Most specific for BVD • Can identify heterozygous carrier
BEST Vitteliform dystrophy • Management • No current medical treatment available • Low vision aids if needed • Genetic and psychological counseling