Download
1 / 1
10 likes | 86 Views
Multi-Level Decision Support (Margie Eastwood / Jean White).

E N D
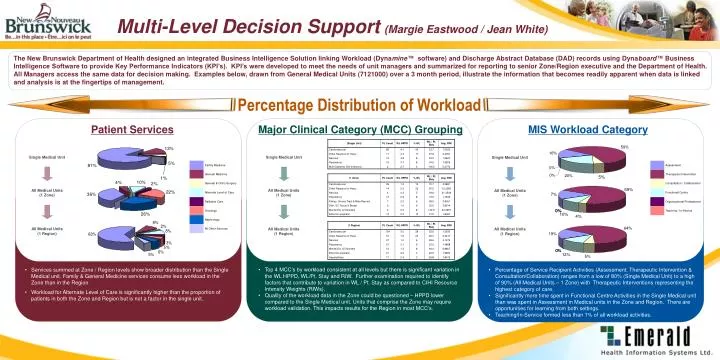
Multi-Level Decision Support(Margie Eastwood / Jean White) The New Brunswick Department of Health designed an integrated Business Intelligence Solution linking Workload (Dynamine™ software) and Discharge Abstract Database (DAD) records using Dynaboard™ Business Intelligence Software to provide Key Performance Indicators (KPI’s). KPI’s were developed to meet the needs of unit managers and summarized for reporting to senior Zone/Region executive and the Department of Health. All Managers access the same data for decision making. Examples below, drawn from General Medical Units (7121000) over a 3 month period, illustrate the information that becomes readily apparent when data is linked and analysis is at the fingertips of management. Percentage Distribution of Workload Patient ServicesMajor Clinical Category (MCC) GroupingMIS Workload Category Single Medical Unit Single Medical Unit Single Medical Unit All Medical Units (1 Zone) All Medical Units (1 Zone) All Medical Units (1 Zone) All Medical Units (1 Region) All Medical Units (1 Region) All Medical Units (1 Region) • Top 4 MCC’s by workload consistent at all levels but there is significant variation in the WL HPPD, WL/Pt. Stay and RIW. Further examination required to identify factors that contribute to variation in WL / Pt. Stay as compared to CIHI Resource Intensity Weights (RIWs). • Quality of the workload data in the Zone could be questioned – HPPD lower compared to the Single Medical unit. Units that comprise the Zone may require workload validation. This impacts results for the Region in most MCC’s. • Services summed at Zone / Region levels show broader distribution than the Single Medical unit. Family & General Medicine services consume less workload in the Zone than in the Region. • Workload for Alternate Level of Care is significantly higher than the proportion of patients in both the Zone and Region but is not a factor in the single unit. • Percentage of Service Recipient Activities (Assessment, Therapeutic Intervention & Consultation/Collaboration) ranges from a low of 80% (Single Medical Unit) to a high of 90% (All Medical Units – 1 Zone) with Therapeutic Interventions representing the highest category of care. • Significantly more time spent in Functional Centre Activities in the Single Medical unit than was spent in Assessment in Medical units in the Zone and Region. There are opportunities for learning from both settings. • Teaching/In-Service formed less than 1% of all workload activities.