Download
1 / 8
80 likes | 160 Views
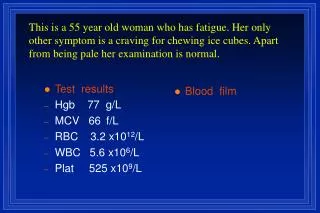
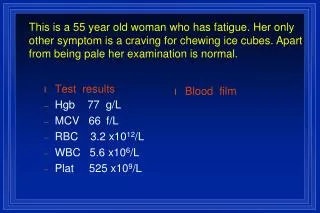
Select each exam or test to learn more about TK’s results. Physical examination. Laboratory tests. Additional laboratory tests. Physical Examination.

E N D
Select each exam or test to learn more about TK’s results. Physical examination Laboratory tests Additional laboratory tests
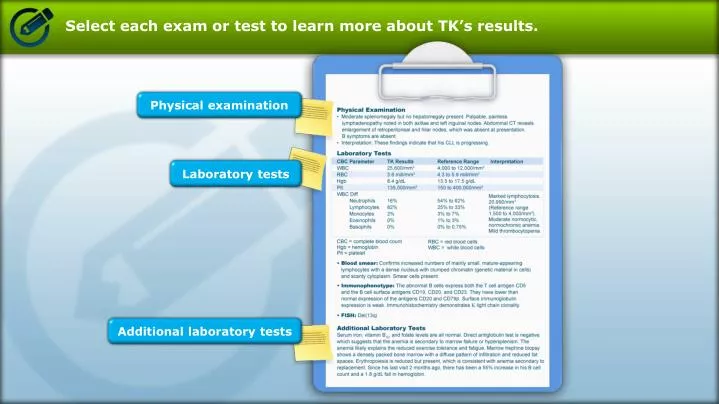
Physical Examination • Moderate splenomegaly but no hepatomegaly present. Palpable, painless lymphadenopathy noted in both axillae and left inguinal nodes. Abdominal CT reveals enlargement of retroperitoneal and hilar nodes, which was absent at presentation. B symptomsare absent. • Interpretation: These findings indicate that his CLL is progressing.
Laboratory Tests • Interpretation: Marked lymphocytosis 20,990/mm3(Reference range 1,500 to 4,000/mm3). Moderate normocytic, normochromic anemia. Mild thrombocytopenia. • Blood smear: Confirms increased numbers of mainly small, mature-appearing lymphocytes with a dense nucleus with clumped chromatin (genetic material in cells) and scanty cytoplasm. Smear cells present. • Immunophenotype: The abnormal B cells express both the T cell antigen CD5 and the B cell surface antigens CD19, CD20 and CD23. They have lower than normal expression of the antigens CD20 and CD79β. Surface immunoglobulin expression is weak. Immunohistochemistry demonstrates Κlight chain clonality. • FISH: Del(13q)
Additional Laboratory Tests Serum iron, vitamin B12, and folate levels are all normal. Direct antiglobulin test is negative, which suggests that the anemia is secondary to marrow failure or hypersplenism. The anemia likely explains the reduced exercise tolerance and fatigue. Marrow trephine biopsy shows a densely packed bone marrow with a diffuse pattern of infiltration and reduced fat spaces. Erythropoiesis is reduced but present, which is consistent with anemia secondary to replacement. Since his last visit 2 months ago, there has been a 55% increase in his B cell count and a 1.8 g/dL fall in hemoglobin.
Select the patient population to learn more about treatment options. With or without del(11p) or without del(17p) and age ≥70 years With or without del(11p) or without del(17p) and age <70 years or older patients without significant comorbidities With del(17p), regardless of age This training is for background purposes only. Superiority claims or comparisons between products can not be made without well controlled, head to head studies.
With or without del(11q) or without del(17p) and age ≥70 years • Chemoimmunotherapy • reduced-dose FCR • reduced-dose PCR • bendamustine ± rituximab • high-dose methylprednisolone (HDMP) + rituximab • chlorambucil ± rituximab • Ofatumumab • Lenalidomide ± rituximab • Alemtuzumab ± rituximab • Dose-dense rituximab
With or without del(11q) or without del(17p) and age <70 years or older patients without significant comorbidities • Chemoimmunotherapy • Ofatumumab • FCR • Lenalidomide ± rituximab • PCR • Alemtuzumab ± rituximab • bendamustine ± rituximab • HDMP + rituximab • RCHOP (rirituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) • R-HyperCVAD (rituximab, cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with high-dose methotrexate and cytarabine) • dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, rituximab) • OFAR (oxaliplatin, fludarabine, cytarabine, rituximab)
With del(17p), regardless of age • Alemtuzumab ± rituximab • RCHOP • CFAR (cyclophosphamide, fludarabine, alemtuzumab, rituximab) • HDMP + rituximab • R-HyperCVAD • Ofatumumab • Lenalidomide ± rituximab • OFAR