Download
1 / 24
250 likes | 597 Views
Reformation of Suture Following Surgery for Isolated Sagittal Craniosynostosis. Deepak Agrawal, Paul Steinbok, D Cochrane Division of Pediatric Neurosurgery, UBC and BC Children’s Hospital, Vancouver, BC. ISOLATED SAGITTAL CRANIOSYNOSTOSIS. BASIS FOR MANAGEMENT

E N D
Reformation of Suture Following Surgery for Isolated Sagittal Craniosynostosis Deepak Agrawal, Paul Steinbok, D Cochrane Division of Pediatric Neurosurgery, UBC and BC Children’s Hospital, Vancouver, BC
ISOLATED SAGITTAL CRANIOSYNOSTOSIS BASIS FOR MANAGEMENT • Isolated entity in a normal child • Operative Intervention-Improve cosmesis
ETIOLOGY Moss’s Hypothesis • Abnormality at cranial base Moss, M. L. (1959). "The pathogenesis of premature cranial synostosis in man." Acta Anat (Basel)37: 351-70. • Proven for syndromic craniosynostosis
ETIOLOGY Babler’s Hypothesis • Abnormality is in the affected calvarial sutures Babler, W. J., J. A. Persing, et al. (1982). "Compensatory growth following premature closure of the coronal suture in rabbits." J Neurosurg57(4): 535-42. • Support from animal experiments Mabbutt, L. W. and V. G. Kokich (1979). "Calvarial and sutural re-development following craniectomy in the neonatal rabbit." J Anat129(2): 413-22.
Reformation of sagittal suture should similarly be expected in children with isolated sagittal synostosis
OBJECTIVE • To determine the incidence of reformation of the sagittal suture following surgical procedures for sagittal synostosis that involved a minimum of sagittal strip craniectomy
MATERIALS AND METHODS • Retrospective study 1987-2000 • Children with isolated sagittal craniosynostosis
Operative Procedure Minimum of vertex and parietal craniectomies (removal of the sagittal suture + 1.5 - 2.5 cm piece of adjacent parietal bone with the attached pericranium) Children who had the bone flap replaced were excluded from the study
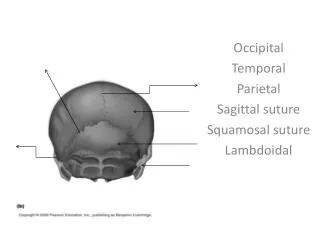
Assessment of resynostosis POST-OP SKULL RADIOGRAPHS • Suture morphology • Patency of coronal and lambdoid sutures
RESULTS • 114 children operated for isolated sagittal craniosynostosis in the above period. • 42 children composed the study group.
RESULTS • Median age at surgery- 3.9 months (1.9 to 7.6 months) • Mean follow up - 32.2 months (6 to 144 months)
RESULTS • Only 7/42 (16.7%) reformed the suture • 35/42 (83.3%) had resynostosis of the sagittal suture
These findings are contrary to the results from animal experiments WHY THE DISCREPANCY?
DISCUSSION • Both dura mater and pericranium have osteogenic properties • Dura-source of central new bone • Pericranium- enhances peripheral new bone formation Gosain AK, Santoro TD, Song LS, et al: Osteogenesis in calvarial defects: contribution of the dura, the pericranium, and the surrounding bone in adult versus infant animals. Plast Reconstr Surg 112:515-527, 2003
DISCUSSION • In Sag synostosis surgery-central strip of bone with the attached pericranium removed • Removal of this pericranium could potentially impair bony regeneration as well as suture reformation
DISCUSSION • Common practice to coagulate the bleeding points on the dura • This again could impair the osteogenic capacity of the dura
DISCUSSION • Primary aim of surgery is cosmetic • Persistence of bony defects and uneven contour of the bony regrowth may result in patient dissatisfaction, rarely culminating in repeat surgery
OUR HYPOTHESIS Limiting coagulation on the dura & replacing pericranium could potentially result in consistent bone regeneration with smooth contour and reformation of a normal suture. Further prospective studies would be required to prove this hypothesis
OTHER POTENTIAL FACTORS GENETIC BASIS • Inclusion of undiagnosed syndromic patients • Genetic predisposition to synostosis
CONCLUSIONS • We found a very high incidence of resynostosis following surgery for sagittal craniosynostosis • The variability in reformation of the suture after surgery suggests a heterogeneous etiology and pathogenesis of isolated sagittal synostosis.