Download
1 / 25
250 likes | 269 Views
Explore the impact of thrombolysis on functional outcome in patients with submassive pulmonary embolism. Studies and findings on RV function, hemodynamic responses, and long-term benefits of thrombolytic therapy. Comparison with heparin treatment.

E N D
Does thrombolysis improve the long-term functional outcome of patients with submassive PE? Cindy Hsu PGY-3 1/16/2013
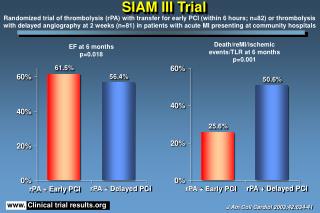
Studies • Sharma GV et al (2000). Long-term benefit of thrombolytic therapy in patients with pulmonary embolism. Vasc Med. 5(2):91-5. • Kline JA et al (2009). Prospective evaluation of right ventricular function and functional status 6 months after acute submassive pulmonary embolism: frequency of persistent or subsequent elevation in estimated pulmonary artery pressure. Chest, 136, pp. 1202–1210 • Fasullo S et al (2011). Six-month echocardiographic study in patients with submassive pulmonary embolism and right ventricle dysfunction: comparison of thrombolysis with heparin. Am J Med Sci. 2011 Jan;341(1):33-9. • Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; “MOPETT” Investigators. Moderate Pulmonary Embolism Treated With Thrombolysis (from the "MOPETT" Trial) (2013). Am J Cardiol. Volume 111, Issue 2, 15 January 2013, Pages 273–277
Definition of submassive PE Acute PE without systemic hypotension (SBP >90 mm Hg) but with either RV dysfunction or myocardial necrosis RV dysfunction: 1. RV/LV > 0.9 on TTE or CT, or RV systolic dysfunction on TTE 2. BNP > 90 pg/mL 3. pro-BNP > 900 pg/mL 4. EKG changes: new complete or incomplete RBBB, anteroseptal STE or STD, or anteroseptal TWIs Myocardial necrosis: Trop I >0.4 ng/mL or Trop T >0.1 ng/mL Jaff et al. 2012 AHA Scientific Guidelines
Sharma et al. (2000) Prospective, randomized study: A total of 23 of the 40 patients from the UPET and USPET studies who had angiographically proven PE and had initially been randomized to an IV infusion of heparin (n = 11) or a thrombolytic agent (urokinase or streptokinase, n = 12) were restudied after a mean follow-up of 7.4 years to measure the right-sided pressures and to evaluate their response to exercise during supine bicycle ergometry.
Sharma et al. (2000) • At rest, the baseline PA mean pressure and PVR were significantly higher in the heparin group • On exercise, the PA mean pressure increased to 32 ± 2.0 mmHg from the resting value of 22 ± 1.4 mmHg (p < 0.01) in the heparin group. There was no significant change (from 17 ± 1.3 to 19 ± 1.4 mmHg; p = NS) in the thrombolytic group. • In the heparin group, PVR was 351 ± 24 dynes s-1cm-5 at rest and increased to 437 ± 30 on exercise (p < 0.01); in the thrombolytic population the corresponding values were 171 ± 16 and 179 ± 18 dynes s-1cm-5, respectively (p = NS).
Sharma et al. (2000) Conclusion: Thrombolysis preserves the normal hemodynamic response to exercise in the long term and may prevent recurrences of venous thromboembolism and the development of pulmonary hypertension.
Kline et al. (2009) • Subgroup analysis of a prospective observational study that consisted of 200 subjects with submassive PE treated with heparin • Measure noninvasively by TTE 6 month from the diagnosis: 1. Change in RV size, function, and RVSP 2. NYHA score and 6-min walk distance (6MWD)
Kline et al. (2009) • Indications for alteplase therapy: circulatory shock (n=10), respiratory failure (n=7), or both (n=4). Alteplase was infused within 24 h of diagnosis in 18 patients and after 5 h in three patients. • Three of the 21 patients treated with heparin and alteplase went on to undergo either catheter fragmentation (1 patient, who subsequently died) or surgical thrombectomy (2 patients, who both survived). • These patients were sicker than the heparin-only group with worse vitals, mean d-dimer, and higher clot burden
Kline et al. (2009) Pulmonary HTN = RVSP > 40 mm Hg *p < 0.001. †p = 0.25. ‡p = 0.01. §p = 0.88 (Mann-Whitney U test)
A Kline et al. (2009) • Among the patients treated with heparin only who had an increase in RVSP (39 patients; 27%), 18 of 39 patients (46%) had either dyspnea at rest or exercise intolerance. This was in contrast to the absence of worsening of the RVSP in any patient of the thrombolysis group. • Neither the 6MWD nor the distributions of the NYHA scores were significantly different between the treatment groups
Kline et al. (2009) 90% of the survivors of submassive PE treated with heparin and heparin + alteplase exhibited resolution of RV dilation and hypokinesis at the 6-month follow-up A larger proportion of patients treated with heparin and alteplase manifested decreases in RVSP, but this observation may be explained by their higher RVSP at diagnosis. Conclusion: Persistent or worsening tricuspid regurgitation suggestive of pulmonary hypertension occurs at a significant rate after acute submassive PE
Fasullo et al. (2011) • Prospective, double-blinded RCT • 72 patients with first episode of submassive PE with < 6 hrs onset, SBP > 100, RVD on echo, positive CT, and EKG/lab/vital changes were randomized to receive 100 mg of alteplase or placebo with heparin • Echo performed throughout admission, at discharge, and at 3 and 6 months
Fasullo et al. (2011) Bleeding was considered as major if it was fatal, intracranial, required transfusions or intervention for hemodynamic deterioration. All bleeding episodes not fulfilling criteria for major bleeding were considered as minor.
Fasullo et al. (2011) RV dysfunction was significantly reduced in thrombolysis group in comparison with placebo group. The BNP showed a faster reduction in thrombolysis group than placebo group during hospitalization, and 6 days after admission, both groups showed normal values of BNP.
Fasullo et al. (2011) • Conclusion: Thrombolysis group showed a significant early and 6-month improvement of RV function compared to heparin group. The same group also showed significant reduction in clinical events during the hospitalization and follow-up.
Sharifi et al. “MOPETT” (2013) Prospective, controlled, randomized, single-center open study that enrolled 121 adult patients with symptomatic “moderate” PE during a 22 month period. Patients were randomized to receive a “safe dose” of 50mg tissue plasminogen activator plus anticoagulation (thrombolysis group [TG], n = 61) or anticoagulation alone (control group [CG], n = 60). Primary end points: pulmonary hypertension and the composite end point of pulmonary hypertension and recurrent PE at 28 months. Secondary end points: total mortality, the duration of hospital stay, bleeding at the index hospitalization, recurrent PE, and the combination of mortality and recurrent PE.
Sharifi et al. “MOPETT” (2013) Inclusion criteria: 1. >70% involvement of thrombus in > 2 lobar or L or R main pulmonary arteries or by high probability V/Q scan showing mismatches in > 2 lobes AND 2. Minimum of ≥ 2 new signs and symptoms: chest pain, tachypnea (RR at rest ≥22), tachycardia (HR at rest ≥90), dyspnea, cough, oxygen desaturation (O2sat <95% ) or elevated JVP ≥12 cm H2O RV enlargement or hypokinesia and elevation of biomarkers of RV injury (trop I and BNP), although measured, were not a requirement for enrollment. (~20% with RV dilation, ~5% with RV dysfunction, and elevated BNP or trop in ~70% in both groups)
Sharifi et al. “MOPETT” (2013) Conclusion: “Safe dose” thrombolysis is safe and effective in the treatment of moderate PE, with a significant immediate reduction in the pulmonary artery pressure that was maintained at 28 months
HUPism • For patients with newly diagnosed PE, order EKG, trop, BNP, and obtain a TTE to evaluate for RV dysfunction or myocardial necrosis • For submassive PE patients with evidence of RV dysfunction or myocardial necrosis, consider the administration of thrombolytics in addition to standard anticoagulation to improve their long-term functional outcome
AHA guidelines Class IIa Class IIb Class IIa Jaff et al. 2012
Keep an eye out for these RCTs! Clot Dissolving Treatment for Blood Clots in the Lungs (Tenecteplase + Enoxaparin, Jeff Kline) PEITHO Pulmonary Embolism Thrombolysis Study (Tenecteplase + heparin, European study) Low Dose Rt-PA for Acute Normotensive Pulmonary Embolism With RVD (50mg Alteplase + LMWH, Chinese study) www.clinicaltrials.gov
References • Jaff et al. (2012) Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011 Apr 26;123(16):1788-830. • Sharma GV, Folland ED, McIntyre KM, Sasahara AA. (2000). Long-term benefit of thrombolytic therapy in patients with pulmonary embolism. Vasc Med. 5(2):91-5. • Kline JA, Steuerwald MT, Marchick MR, Hernandez-Nino J, Rose GA (2009). Prospective evaluation of right ventricular function and functional status 6 months after acute submassive pulmonary embolism: frequency of persistent or subsequent elevation in estimated pulmonary artery pressure. Chest, 136, pp. 1202–1210 • Fasullo S, Scalzo S, Maringhini G, Ganci F, Cannizzaro S, Basile I, Cangemi D, Terrazzino G, Parrinello G, Sarullo FM, Baglini R, Paterna S, Di Pasquale P (2011). Six-month echocardiographic study in patients with submassive pulmonary embolism and right ventricle dysfunction: comparison of thrombolysis with heparin. Am J Med Sci. 2011 Jan;341(1):33-9. • Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; “MOPETT” Investigators. Moderate Pulmonary Embolism Treated With Thrombolysis (from the "MOPETT" Trial) (2013). Am J Cardiol. Volume 111, Issue 2, 15 January 2013, Pages 273–277