Download
1 / 40
400 likes | 413 Views
Intestinal Metaplasia of the Stomach. A Review. Kent Humble MD Assistant Professor of Family Medicine LSU School of Medicine. Objectives. Discuss relationship between gastric IM and gastric cancer. Review pathophysiology and epidemiology of gastric IM.

E N D
Intestinal Metaplasia of the Stomach A Review Kent Humble MD Assistant Professor of Family Medicine LSU School of Medicine
Objectives Discuss relationship between gastric IM and gastric cancer Review pathophysiology and epidemiology of gastric IM Review guidelines concerning endoscopic surveillance
US Incidence by Ethnic Background 2008 Int J Cancer 2010;127(12):2893
Highest incidence in East Asia, Eastern Europe, and Western South America
Intestinal Type Diffuse Type
Gastric Cancer • Diffuse Type • 20-30% of cases • Uniform across countries • Younger age (mean 38) • No identified precursors • Male to Female 1:1 Intestinal Type 70-80% of cases Predominantly in high risk areas Develops from precursors Male to Female 2:1 Older age (mean 69) Environmental factors Genetic factors
Intestinal Metaplasia Atrophic Gastritis Cancer Gastritis Dysplasia Correa Progression Gastric IM is likely the 'breaking point' between chronic gastritis and dysplasia
Am J Physiol Gastrointest Liver Physiol 291: G999 –G1004, 2006
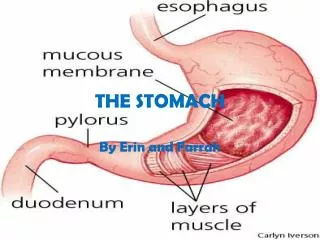
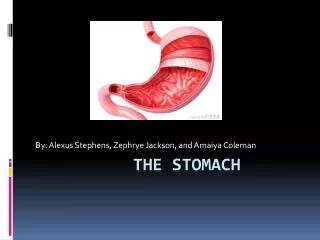
What is Gastric IM? • Foci appear at junction of Antrum & Body, often at Angularis • Enlarge, coalesce, extending to Antrum & Body • Small foci of dysplasia may appear in areas of IM, subject to sampling error • Severity & tempo of progression may be influenced by virulence of H Pylori (?cagA), environmental, host genetic factors
EPIDEMIOLOGY OF IM Found in up to 25% US Adults 13% of Caucasians 50% of Blacks/Hispanics H. pylori infection significantly raises IM prevalence Increases with patient age Higher in first degree relatives with gastric cancer Cancer Epidemiol Biomarkers Prev 1992;1:293–296.
EPIDEMIOLOGY OF IM • Systematic review: Patients with IM Gastric cancer incidence varied 0-10% Am J Surg Pathol 2000; 24: 167-176 • Dutch study: Histology based • 61,707 pts with IM • 874 developed gastric CA over 10 years • 0.18%yearly Gastroenterology 2008; 134: 945-952
ARE ALL PATIENTS WITH IM AT EQUAL RISK OF GASTRIC CANCER? The presence of incomplete-type IM is associated with a higher gastric cancer risk compared to complete-type IM. Spain study: Mean follow-up 12.8 years • Incomplete IM: 16 of 88 pts (18.2%) developed gastric CA • Complete IM: 1 of 104 pts (0.96%) developed gastric CA Int J Cancer 2010; 127: 2654-2660
ARE ALL PATIENTS WITH IM AT EQUAL RISK OF GASTRIC CANCER? Gastric cancer risk is associated with IM topography. Columbia study: Compared to antral predominate (focal) • Extension through angularis- risk 5.7 fold • Antrum plus body (diffuse)- risk 12.2 fold Incomplete IM presents as diffuse more commonly than focal Am J Gastroenterol 2000; 95: 1431-1438
ARE ALL PATIENTS WITH IM AT EQUAL RISK OF GASTRIC CANCER? Extensive IM increases the risk of progression to dysplasia. Italian Study • The rate of gastric cancer appeared to increase with increasing IM extension Hum Pathol 2006; 37 1489-1497 IM may be considered extensive when it involves at least two locations or when it is moderate or marked in more than one biopsy specimen
IS IM REVERSIBLE? H. pylori eradication may slow IM progression. Hong Kong Study • 537 pts with IM and H. Pylori randomized to treatment or placebo • H Pylori eradication prevented IM progression • Odds ratio 0.48 (95% CI: 0.32-0.74) Gut 2004; 53: 1244-1249
IS IM REVERSIBLE? IM does not appear to regress following H. pylori eradication. Meta-analysis of 7 studies • Unlike atrophy, no significant IM regression occurred following H. Pylori eradication Helicobacter 2007; 12 Suppl 2: 32-38 Meta-analysis of 12 studies • Atrophy improved in the body but not antrum • IM did not improve after eradication Digestion 2011; 83: 253-260
IS IM REVERSIBLE? Italian Study • 6 months of ascorbic acid qOD following H. Pylori eradication helped reduce IM Aliment Pharma- col Ther 2000; 14: 1303-1309 Taiwan Study • IM regressed in 24% of 33 pts following 8 wks of treatment with celecoxib 200 mg/d after H. Pylori eradication J Gastroenterology Hepatol 2010; 25: 48-53
What About Surveillance? Dutch study: Can extension be predicted? 88 patients with previous IM on gastric biopsy Repeat EGD & blood tests done • Most important predictors of extensive IM: • Family history of gastric cancer • Alcohol use 10ml per day • Marked IM of index biopsy • Pepsinogen I/II ratio < 3.0 Gastrointestinal Endoscopy Vol 70, No.1:2009
PG I & II PG II PG II
2006 ASGE Guideline • Endoscopic surveillance for gastric intestinal metaplasia has not been extensively studied in the U.S. and therefore cannot be uniformly recommended • Patients at increased risk for gastric cancer due to ethnic background or family history may benefit from surveillance • Endoscopic surveillance should incorporate topo- graphic mapping of the entire stomach Gastrointestinal Endoscopy Volume 63, No. 4 : 2006
2012 European Guideline • Conventional white light endoscopy cannot accurately differentiate between benign and precancerous gastric conditions/lesions • Magnification chromoendoscopy (MCE) or narrow-band imaging (NBI) endoscopy with or without magnification may be offered in these cases as it improves diagnosis of such lesions • At least four non-targeted biopsies of the proximal and distal stomach, on the lesser and greater curvatures, are needed for adequate assessment of premalignant gastric conditions Virchows Arch. 2012 Jan;460(1):19-46. Epub 2011 Dec 22.
2012 European Guideline • Patients with extensive atrophy and/or extensive IM should be offered endoscopic surveillance every 3 years • Further studies are needed however, to accurately estimate the cost–effectiveness of such an approach • Patients with mild to moderate atrophy/IM only in Antrum do not need follow-up • Sub-typing of IM is not recommended for clinical practice Virchows Arch. 2012 Jan;460(1):19-46. Epub 2011 Dec 22.
2012 European Guideline • COX-2 inhibitors, or the use of dietary supplementation with antioxidants (ascorbic acid and beta-carotene) are not endorsed as approaches to decrease the risk of progression of gastric precancerous lesions • Neither age, gender, H. pylori virulence factors, or host genetic variations change these clinical recommendations Virchows Arch. 2012 Jan;460(1):19-46. Epub 2011 Dec 22.
2012 European Guideline Virchows Arch. 2012 Jan;460(1):19-46. Epub 2011 Dec 22. IM may be considered extensive when it involves at least two locations or when it is moderate or marked in more than one biopsy specimen
What's new? OLGA Operative Link for Gastritis Assessment OLGIM Operative link on Gastric Intestinal Metaplasia Assessment. Gastritis staging systems that arrange histological phenotypes of gastritis along a scale of progressively increasing gastric cancer risk, from the lowest (stage 0) to the highest (stage IV).
Thank You khumbl@lsuhsc.edu