Download
1 / 77
830 likes | 1.29k Views
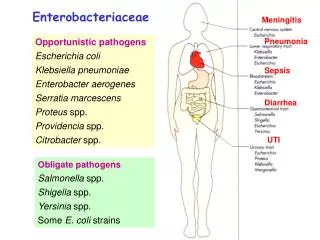
Enterobacteriaceae. Shigella. E. coli. Providencia. Transmitted by the fecal-oral route. Salmonella. Morganella. Klebsiella pneumoniae. Enterobacter. Yersinia. Primary pathogens Organisms capable of causing disease in anyone.

E N D
Shigella E. coli Providencia Transmitted by the fecal-oral route Salmonella Morganella Klebsiellapneumoniae Enterobacter Yersinia Primary pathogensOrganisms capable of causing disease in anyone Opportunistic pathogensOrganisms that can only cause disease under certain conditions or in certain hosts Proteus Senatia
Characteristics shared by all members of family Enterobacteriaceae
Peritrichous flagella -shigella: nonmotile Facultative anaerobe Not fastidious
Active metabolism - All ferment glucose; - All reduce nitrates to nitrites; - All oxidase negative - Lactose fermentation: the key measure to isolate and identify the Enterobacteriaceae +: nonpathogenic -: pathogenic
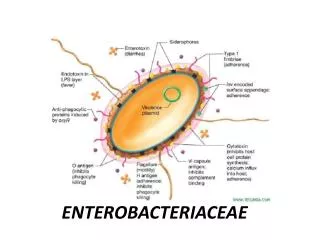
Antigenic structures • LPS (endotoxin) –O antigen. • Most are motile by peritrichous flagella --H antigens. • Capsule – Kantigen (Vifor Salmonella). • Cell envelope (wall) • various outer membrane proteins. • Pili - various antigen types, some encoded by plasmids
Enterobacteriaceae:gastrointestinal diseases • Escherichia coli • Salmonella • Shigella • Yersinia entercolitica
Serotypes • reference laboratory • antigens • O (lipopolysaccharide) • H (flagellar) • K (capsular) O6:K15:H6
Normal flora pathogen Opportunistic pathogen E. coli is the majority of GI normal flora Intestinal tract infection ETEC EIEC EPEC EHEC EAggEC Extraintestinal infection Urinary tract infection Septicemia Neonatal meningitis Medical significance
Escherichia coli • Toxins: two types of enterotoxin; Shiga-type toxin; Enteroaggregative ST-like toxin; Hemolysins; Endotoxin • Type III secretion system • Adhesions: colonization factors ; both pili or fimbriae; non-fimbrial factors involved in attachment. There are at least 21 different types of adhesions. • Virulence factors that protect the bacteria from host defenses: Capsule/Iron capturing ability (enterochelin) • Outer membrane proteins
What is the pathogenesis of these five groups of pathogenic E. coli? Gastroenteritis caused by E. coli
Enterotoxigenic E. coli (ETEC) • A watery diarrhea, nausea, abdominal cramps and low-grade fever for 1-5 days. • Travellers diarrhea and diarrhea in children in developing countries • Transmission is via contaminated food or water. • diarrhea like cholera • milder • nursery travellers diarrhea • caused by LT, ST, or LT/ST.
Enterotoxigenic E. coli (ETEC) • Heat labile toxin • like choleragen • Adenyl cyclase activated • cyclic AMP • secretion water/ions • Heat stable toxin • Guanylate cyclase activated • cyclic GMP • uptake water/ions
Enteroinvasive E. coli (EIEC) • The organism attaches to the intestinal mucosa via pili • Outermembrane proteins are involved in direct penetration, invasion of the intestinal cells, and destruction of the intestinal mucosa. • There is lateral movement of the organism from one cell to adjacent cells. • Symptoms include fever, severe abdominal cramps, malaise, and watery diarrhea followed by scanty stools containing blood, mucous, and pus. • resembles shigellosis
Enteroinvasive E. coli (EIEC) • Dysentery • rearrangement of intracellular actin • resembles shigellosis • elder children and adult diarrhea
Enteropathogenic E. coli (EPEC) • Malaiseand low grade feverdiarrhea, vomiting, nausea, non-bloody stools • Bundle forming pili are involved in attachment to the intestinal mucosa. • This leads to changes in signal transduction in the cells, effacement of the microvilli, and to intimate attachment via a non-fimbrial adhesion called intimin. • This is a problem mainly in hospitalized infants and in day care centers.
Enteropathogenic E. coli (EPEC) • fever • infant diarrhea • vomiting • nausea • non-bloody stools • Destruction of surface microvilli - loose attachment mediated by bundle forming pili (Bfp); - Stimulation of intracellular calcium level; - Rearrangement of intracellular actin
Enterohemorrhagic E. coli (EHEC) • Hemorrhagic • bloody, copious diarrhea • few leukocytes • afebrile • Hemolytic-uremic syndrome • hemolytic anemia • thrombocytopenia (low platelets) • kidney failure
Enterohemorrhagic E. coli (EHEC) • Vero toxin • “shiga-like” • Hemolysins • younger than 5 years old,causing hemorrhagic colitis
Transmission electron micrograph Enterohemorrhagic E. coli (EHEC) • Usually O157:H7
Enteroaggregative E. coli (EaggEC) • a cause of persistent, watery diarrhea with vomiting and dehydration in infants. • That is autoagglutination in a ‘stacked brick’ arrangement. • the bacteria adheres to the intestinal mucosa and elaborates enterotoxins (enteroaggregative heat-stable toxin, EAST). • The result is mucosal damage, secretion of large amounts of mucus, and a secretory diarrhea.
Enteroaggregative E. coli (EaggEC) • Mucous associated autoagglutinins cause aggregation of the bacteria at the cell surface and result in the formation of a mucous biofilm. • The organisms attach via pili and liberate a cytotoxin distinct from, but similar to the ST and LT enterotoxins liberated by ETEC. • Symptoms incluse watery diarrhea, vomiting, dehydration and occasional abdominal pain.
“Nonintimate” association: bacteria attach to host cell by bundle-forming pili Bacterial attachment: signal transduction event stimulated; host cell tyrosine kinase activated; Ca2+ levels increase “Intimate” contact: pedestallike structure (composed of actin fibers) forms in host cell under bacteria (intimin)
Escherichia coli • In the diagnostic laboratory generally the groups are not differentiated and treatment would be on symptomatology. • Generally fluid replacement is the primary treatment. • Antibiotics are generally not used except in severe disease or disease that has progressed to a systemic stage (e.g.hemolytic-uremia syndrome). • Two major classes of pili are produced by E. coli : mannose sensitive and mannose resistant pili. The former bind to mannose containing glyocoproteins and the latter to cerebrosides on the host epithelium allowing attachment. This aids in colonization by E. coli.
Sanitary significance • Total bacterial number: number of bacteria contained per ml or gm of the sample; the standard of drinking water is less than 100. • Coliform bacteria index: the number of coliform bacteria detected out per 1000 ml sample; the standard of drinking water is less than 3
Genral features • Pili. • Most strains can not ferment lactose; S. sonnei can slowly ferment lactose. • According to O antigen, 4 groups • Easily causing drug-resistence.
What disease is caused by Shigella species? Bacillary dysentery shigellosis
Bacillary dysentery • Source - humans are the only reservoir • Transmission - the fecal-oral route • Clinical findings -watery diarrhea -abdominal cramps -tenesmus -bloody stool with mucus and pus -fever • Clinical types - acute dysentery acute toxic dysentery -chronic dysentery
Shigellosis • within 2-3 days • epithelial cell damage • bloody feces • intestinal pain • pus
Shigellosis • Invasiveness • Endotoxin • Exotoxin: Shiga toxin - S. dysenteriae - neurotoxic, enterotoxic and cytotoxic
Shiga toxin • enterotoxic • cytotoxic • inhibits protein synthesis • lysing 28S rRNA
Clinical significance • man only "reservoir" • mostly young children • fecal to oral contact • children to adults • transmitted by adult food handlers • unwashed hands
Clinical significance • The infective dose required to cause infection is very low (10-200 organisms). • There is an incubation of 1-7 days followed by fever, cramping, abdominal pain, and watery diarrhea (due to the toxin)for 1-3 days. • This may be followed by frequent, scant stools with blood, mucous, and pus (due to invasion of intestinal mucosa). • Is is rare for the organism to disseminate. • The severity of the disease depends upon the species one is infected with. S. dysenteria is the most pathogenic followed by S. flexneri, S. sonnei and S. boydii.
immunity • Primary immunity defense - SIgA • Immunity intensity - Limited - reasons surface infection various types
Diagnosis of Shigella infection • Specimen:stool. • Culture and Identification • Quick immunological methods: - Immunofluorescent “ball” test; - Coagglutination.
Prevention & Treatment • manage dehydration • patients respond to antibiotics , Problem of drug-resistance • disease duration diminished • streptomycin dependent (SD) dysentery vaccine.
Summary Shigella • Shigella (4 species; S. flexneri, S. boydii, S. sonnei, S. dysenteriae) all cause bacillary dysentery or shigellosis, (bloody feces associated with intestinal pain). • The organism invades the epithelial lining layer, but does not penetrate. • Usually, within 2-3 days, dysentery results from bacteria damaging the epithelium lining layers of the intestine often with release of mucus and blood (found in the feces) and attraction of leukocytes (also found in the feces as "pus").
Summary Shigella • Shiga toxin (chromosomally encoded) is neurotoxic, enterotoxic and cytotoxic plays a role. The toxin inhibits protein synthesis (acting on the 80S ribosome and lysing 28S rRNA). • This is primarily a disease of young children occurring by fecal-oral contact. Adults can catch this disease from children. However it can be transmitted by infected adult food handlers, contaminating food. The source in each case is unwashed hands. Man is the only "reservoir". • Patients with severe dysentery are usually treated with antibiotics (e.g. ampicillin). In contrast to salmonellosis, patients respond to antibiotic therapy and disease duration is diminished.