Download
1 / 29
320 likes | 1.21k Views
Pelvic Girdle. 1 st year 1 st quarter. HIP. *AP affected hip **If this is the initial exam of the hip you might need to take a AP pelvis instead of a AP hip *Lateral affected hip. Structures shown AP Hip.

E N D
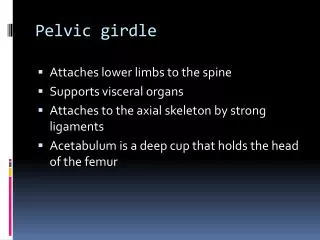
Pelvic Girdle 1st year 1st quarter
HIP *AP affected hip **If this is the initial exam of the hip you might need to take a AP pelvis instead of a AP hip *Lateral affected hip
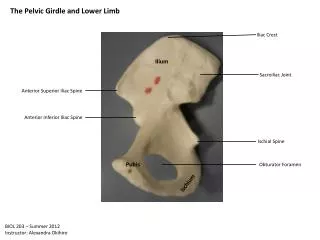
Structures shownAP Hip • Head, neck, trochanters and proximal one third of the body of the femur. *The pubic symphysis must be shown on one view of the hip
Good Film • Lower portion of the ilium and pubic symphysis should be included on the film. • Any orthopedic appliance should be included in its entirety • The greater trochanter should be in profile • The long axis of the femoral neck should be seen • The proximal third of the femur should be included • Little or none of the lesser trochanter should be visible beyond the medial edge of the femur
AP Right Hip pubic symphysis Neck greater trochanter Lesser trochanter
Bursitis AP Right Hip
Structures shownLateral hip(mediolateral Lauenstein method) • A lateral projection of the hip is demonstrated, showing the acetabulum, the proximal end of the femur, and the relationship of the femoral head to the acetabulum
Good Film • ***Don’t do this view if fracture is likely or patient is post-op for less than three days. • The hip joint should be centered to the film. • The hip joint, acetabulum, and femoral head should be well demonstrated.
Hip pinning Lateral Right Hip
Lateral Right Hip End of hardware Plug
Lateral Right Hip Extra bone formation after surgery
Pediatric Patients: Congenital Hip Abnormalities • AP pelvis • Modified Cleaves (***not done if fracture is suspected)
“Frog legs” Modified Cleaves method For pediatric patients with congenital hip abnormalities
Structures shownAxiolateral Hip (Danelius-Miller) • Axiolateral projection of the acetabulum and the proximal femur to include the head, neck, and trochanters. *** This view is done to see the neck
Good Film: • Do this view if fracture is likely or patient is post-op. • As much of the femoral neck should be seen as possible without overlap from the greater trochanter • Only a small amount of the lesser trochanter should be seen on the posterior surface of the femur • A small amount of the greater trochanter should be seen on the anterior and the posterior surfaces of the proximal femur (when it is safe for the femur to be inverted) • The soft tissue shadow of the unaffected thigh should not overlap the hip joint or proximal femur. • The hip joint with the acetabulum should be included .
Soft tissue Other leg neck Greater trochanter X-Table Lateral Lt Hip
RT Don’ forget you might have to build your Pt up ! X-Table Lateral Rt Hip
Other leg in the way! X-Table Lateral Rt hip
Judet’s method • RPO • LPO Structures shown: The acetabular rim
Different than Merrill’s: • We want AP oblique position to include both hips on each film.(always do both obliques) The whole pelvis should be included. The iliac wing is also well visualized.
Why would you do them? • Used to demonstrate fractures of the posterior (ilioischial) column and anterior rim of the acetabulum.