Download
1 / 17
170 likes | 356 Views
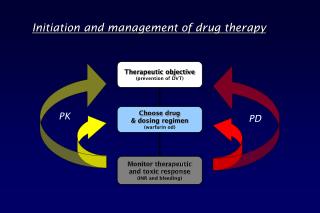
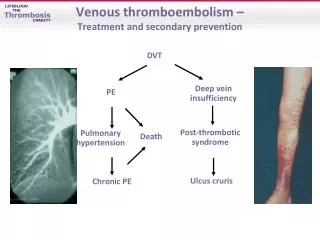
Initiation and management of drug therapy. Therapeutic objective (prevention of DVT). Choose drug & dosing regimen (warfarin od). PK. PD. Monitor therapeutic and toxic response (INR and bleeding). Interpatient variability - Pharmacodynamic factors.

E N D
Initiation and management of drug therapy Therapeutic objective (prevention of DVT) Choose drug & dosing regimen (warfarin od) PK PD Monitor therapeutic and toxic response (INR and bleeding)
Interpatient variability - Pharmacodynamic factors Drug effects in vitro may confirm to simplified schemes. • The concentration-effect seen clinically rarely conforms to these schemes but have 4 characteristic variables: • Potencyaffects dosage but is relatively unimportant. • Maximal effect is NOT equivalent to efficacy and is usually more important than potency. BUT may not be achieved due to concentration-related adverse effects. • Slope is relevant to dose range. • Individual responsiveness (variability) will depend on genetic, age, disease and drug effects on receptor function.
Interpatient Variability - Pharmacokinetic factors: Absorption Generally maximal in upper SB - gastric emptying often rate limiting hence …. AUC increased by metoclopramide/erythromycin and reduced by atropinics, phenthiazines and antihistamines The Effect of food often unpredictable - may (INH, rifampicin or captopril) - or (chloroquine) Drugs with high first-pass (verapamil, propranolol) with food intake Specific effects of certain foods milk/antacids - tetracyclines grapefruit juice -felodipine/terfenadine First-pass metabolism * (inactivation before entering the systemic circulation) gut lumen insulin/benzylpenicillin gut wall tyramine/salbutamol liver propranolol, verapamil, lignocaine * Avoided by alternate route e.g. sl GTN, intranasal insulin, pr ergotamine
Interpatient Variability - Pharmacokinetic factors: Elimination Liver disease (eg cirrhosis) affects first-pass by: (1) direct impairment of hepatocellular function; (2) shunting drug directly into the systemic circulation - increased bioavailability may be huge (eg 10-fold for chlormethiazole) - pro-drug activation may be severely impaired eg ACEIs - concomitant hypoalbuminaemia will complicate the picture if free fraction affects clearance - certain liver diseases have little PK impact eg acute viral hepatitis Renal impairment directly affects renal clearance as well as having indirect effects on protein binding and hepatic metabolism: - only binding of acidic drugs (eg warfarin/phenytoin) are affected HD does not restore reduced albumin binding but transplant does - reduced hepatic clearance (eg propranolol/nicardipine) depends on dialyzable factors in uraemic plasma
Biotransformation of Drugs: 1. Oxidation/Reduction by the P450 system • Haem-containing proteins within the smooth ER responsible for most PHASE I biotransformations • Large superfamily of enzymes - 12 gene families expressed in humans. • Diverse range of xenobiotics are substrates for the P450 system - but all show high lipid solubility. • CYP3A4 is the major isoform in humans with substantial extrahepatic expression especially in the gut wall. Relative contribution of the major P450 isoforms to human drug metabolism
Factors Affecting Metabolism by P450s: (1) INDUCTION by drugs or other environmental chemicals - increased metabolism reduces availability of parent drugs (unless the metabolite is active when induction actually increases availability and toxicity) - generally family specific Agent Isoform Induced polycyclic aromatic hydrocarbons in cigarette smoke CYP1A anticonvulsants CYP3A chronic EtOH, acetone and isoniazid CYP2E1 (2) INHIBITION by concommitant drugs - Competitive antagonism of specfic isoforms eg QUINIDINE (2D6) and FURAFYLLINE (1A2) - Haem-Fe binding eg CIMETIDINE, KETOCONAZOLE, ERYTHROMYCIN. - Suicide inhibitors eg OC (ethinyl oestradiol) and SECOBARB. (3) GENETIC POLYMORPHISMs within the CYP genes. - Subjects show extensive or poor metabolism of drugs transformed through specific P450s. Best characterized for CYP2D6 where PMs make up 10% of Caucasian subjects. Up to 20 alleles known and typable by PCR-RFLP (PHARMACOGENOTYPING).
Clinical Implications of CYP2D6 variants: Agents metabolized by CYP2D6 Cardiovascular Flecainide Metoprolol Propafenone Timolol Mexilitine Propranolol Psychoactive Clozapine Amitriptyline Haloperidol Imipramine Perphenazine Clomipramine Remoxipride Thioridazine PMs show large increases in AUC compared to EMs. The high plasma levels increase the frequency of adverse drug reactions (type I) and reduces drug tolerance in PMs. In the Case of METOTPROLOL, PMs are at high risk of hypotension and bradycardia even at normal ‘therapeutic’ doses. • As well as ‘loss-of-function’ variants, ultrarapidmetabolizers have been identified with duplicated or amplified 2D6 genes. These may explain some incidences of apparent therapeutic ‘failure’ with 2D6 metabolized drugs.
Monitoring drug therapy 1. By Clinical Response Indication result to result to toxic signs dose dose Frusemide Heart Failure Urea Oedema Severe Dehydration hypotension Carbidopa/DOPAParkinson’s Dyskinesias Poor Confusion Blepharospasm Control Depression ThiopentoneInduction Anaesthesia Insufficient Respiratory Too Deep Anaesthesia Failure
Monitoring drug therapy 2. By an in Vitro Test of Therapeutic Effect Indication result to result to toxic signs dose dose Warfarin TE disease high INR low INR Bleeding ThyroxineHypothyroidism low TSH high TSH Hyperthyroidism Statin Raised cholesterol AST/CK high TC Myopathy
Monitoring drug therapy • 3. By a target concentration strategy provided … • Drug level quantitatively correlates with therapeutic & toxic effects. • High risk of therapeutic failure (lack of response or toxicity)* • * Therapeutic failure usually arises if the drug has: • (1) A low therapeutic index • (2) Highly variable pharmacokinetics due to • - saturable elimination • - genetic factors (poor metabolisers) • - concurrent disease • - multiple (and interacting) drug therapies • but remember to confirm compliance in all cases of therapeutic failure
Repeated Drug Dosing to Maintain SS Levels Within a Therapeutic Range Therapeutic Range • Lower limit set by the drug level giving perhaps 50% of the maximum therapeutic effect. • The upper limit is defined by toxicity NOT therapeutic effect and is the level causing toxicity in <5-10% patients.
TDM: Aminoglycosides • Monitoring is mandatory in ALL patients • AG accumulate in the renal cortex to levels 100-fold > plasma • >95% of AG are cleared by glomerular filtration • Toxicity manifests as: • NEPHROTOXICITY(Proximal tubule) • OTOTOXICITY (Hair cells) • Targets for IV GENTAMICIN • peak 30-60 min post-dose = 5-10 mg/L ) BUT toxicity can emerge below these levels • Trough before next dose < 2 mg/L ) if loop diuretics co-administered • If impaired renal function either REDUCE DOSE or INCREASE DOSE INTERVAL • (in anephric patients creatinine clearance = 0 : adjustment, knr/kr = 1/20 so … • dose reduced to 0.25mg/kg/d or interval increased to 160h) cochlear (hearing deficits) - neomycin/amikacin vestibular (disturbed balance) - streptomycin/gentamicin
TDM: Anticonvulsants (PHENYTOIN) • Therapeutic range - 40-80mol/L (NB total drug) • Hypoalbuminaemia and urea both the free fraction • Toxicity - manifests as nystagmus, ataxia and confusion • (dose-dependent in that order) Extensive but saturable hydroxylation in the liver I.e. switches from zero to 1st order elimination within the TR - ‘apparent’ t1/2 may rise from 10-15h to >150h * * dose increments within the TR should be no more than 25-50mg Mild P450 inducer and will increase clearance of: warfarin, OCP, dexamethasone, cyA and pethidine.
TDM: Theophylline • Therapeutic range - 5-20g/ml (28-110mol/L) • Toxicity - manifest as tachyarrythmias, vomiting & convulsions. • PK problems - Bioavailability varies widely between preparations and lower in MR formulations given PM vs. AM. Non-linear CL: 90% eliminated by the liver & 10% unchanged in the urine (reversed ratio in neonates) I.e.No adjustment for renal failure required but dose in presence of impaired hepatocellular function. • Whenever possible establish drug level before administering IV and • if in doubt do not give bolus loading dose. Alteration in Clearance increased decreased rifampicin erythromycin anticonvulsants ciprofloxacin smoking (>10cigs/d) verapamil propranolol
TDM: Lithium • Therapeutic range 0.6-1.2 mmol/L NB at plateau (pre-dose) & avoid Li-heparin tubes! • Toxicity - signs as a guide - TR: fine tremor especially at dosing peak • - moderate intox (1.5-3): coarse tremor, ataxia & diarrhoea • - severe intoxication (>3): confusion & fits • PK problems Complete absorption - SR formulations to reduce peak levels. • >95% excreted by the kidney - initial t1/2 12h • but terminal t1/2 much longer • 70-80% reabsorbed in PCT with no distal • reabsorption (unlike Na) • PCT retention (hence toxicity risk ) is by: • reduced exchangeable Na from any cause • loop or thiazide diuretics • NSAIDs or ACEIs. • Special problemsPregnancy - Dose requirements increase due to renal clearance. Li is also teratogenic and excreted in breast milk • Severe intoxication - usually requires dialysis but because of slow clearance from some compartments rebound rises in Li levels may necessitate repeated HD.
TDM: Digoxin • Therapeutic range 1-2ng/L (taken >6h post-dosing; 1ng/L=1.3nmol/L) for inotropic effect not AF. • Toxicity - may be nonspecific eg nausea, vomiting, abdo pain & confusion but remember bradycardia with increasing of heart block especially with AV junctional escape rhythms and visual disturbance (xanthochromia). • PK problems - 10% population have enteric bacterium (E. lentum) that can metabolize digoxin. Large volume of distribution ( 5L/kg lean BW) and predomin excreted unchanged in the urine with CL GFR. • Large of number of interactions - Mechanism Condition/Drug(s) PK Vd and CL Thyrotoxicosis/T4 Vd and/or CL Verapamil, amiodarone, propafenone absorption Erythromycin, omeprazole absorption Exchange resins, kaolin GFR Any cause of renal impairment/Cyclosporine PD increase block Hypokalaemia/Kaluretic diuretics of the Na pump
Enzyme Induction/inhibition by Anticonvulsants: Phenytoin, phenobarb, CBZ Lamotrigine Valproate Felbamate Ethosuximide Gabapentin Tiagabine Vigabatrine *CYP/UGT UGT (weak) UGT/epoxidases/CYP2C 3A4 2C19 No Effect * =inhibition; / =induction (+/++)