Download
1 / 1
10 likes | 112 Views
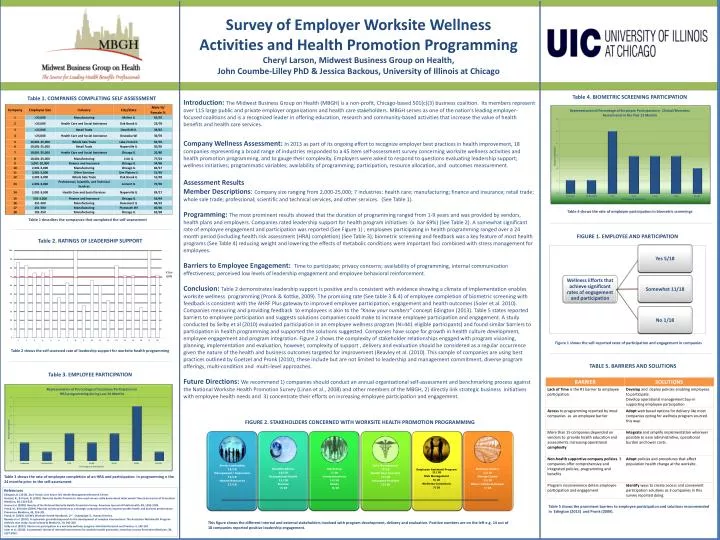
Survey of Employer Worksite Wellness Activities and Health Promotion Programming Cheryl Larson, Midwest Business Group on Health, John Coumbe-Lilley PhD & Jessica Backous , University of Illinois at Chicago. Table 4. BIOMETRIC SCREENING PARTICIPATION.

E N D
Survey of Employer Worksite Wellness Activities and Health Promotion Programming Cheryl Larson, Midwest Business Group on Health, John Coumbe-Lilley PhD & Jessica Backous, University of Illinois at Chicago Table 4. BIOMETRIC SCREENING PARTICIPATION Table 1. COMPANIES COMPLETING SELF ASSESSMENT Introduction: The Midwest Business Group on Health (MBGH) is a non-profit, Chicago-based 501(c)(3) business coalition. Its members represent over 115 large public and private employer organizations and health care stakeholders. MBGH serves as one of the nation’s leading employer-focused coalitions and is a recognized leader in offering education, research and community-based activities that increase the value of health benefits and health care services. Company Wellness Assessment: In 2013 as part of its ongoing effort to recognize employer best practices in health improvement, 18 companies representing a broad range of industries responded to a 45 item self-assessment survey concerningworksite wellness activities and health promotion programming, and to gauge their complexity. Employers were asked to respond to questions evaluating leadership support; wellness initiatives; programmatic variables; availability of programming; participation, resource allocation,and outcomes measurement. Assessment Results Member Descriptions: Company size ranging from 2,000-25,000; 7 industries: health care; manufacturing; finance and insurance; retail trade; whole sale trade; professional; scientific and technical services, and other services. (See Table 1). Programming: The most prominent results showed that the duration of programming ranged from 1-9 years and was provided by vendors, health plans and employers. Companies rated leadership support for health program initiatives (x bar 69%) (See Table 2). A somewhat significant rate of employee engagement and participation was reported (See Figure 1) ; employees participating in health programming ranged over a 24 month period (including health risk assessment (HRA) completion) (See Table 3); biometric screening and feedback was a key feature of most health programs (See Table 4) reducing weight and lowering the effects of metabolic conditions were important foci combined with stress management for employees. Barriers to Employee Engagement: Time to participate; privacy concerns; availability of programming, internal communication effectiveness; perceived low levels of leadership engagement and employee behavioral reinforcement. Conclusion: Table 2 demonstrates leadership support is positive and is consistent with evidence showing a climate of implementation enables worksite wellness programming (Pronk & Kottke, 2009). The promising rate (See table 3 & 4) of employee completion of biometric screening with feedback is consistent with the AHRF Plus gateway to improved employee participation, engagement and health outcomes (Soleret al. 2010). Companies measuring and providing feedback to employees is akin to the “Know your numbers” concept Edington (2013). Table 5 states reported barriers to employee participation and suggests solutions companies could make to increase employee participation and engagement. A study conducted by Selby et al (2010) evaluated participation in an employee wellness program (N=441 eligible participants) and found similar barriers to participation in health programming and supported the solutions suggested. Companies have scope for growth in health culture development, employee engagement and program integration. Figure 2 shows the complexity of stakeholder relationships engaged with program visioning, planning, implementation and evaluation, however, complexity of support , delivery and evaluation should be considered as a regular occurrence given the nature of the health and business outcomes targeted for improvement (Reavley et al. (2010). This sample of companies are using best practices outlined by Goetzel and Pronk (2010), these include but are not limited to leadership and management commitment, diverse program offerings, multi-condition and multi-level approaches. Future Directions: We recommend 1) companies should conduct an annual organizational self-assessment and benchmarking process against the National Worksite Health Promotion Survey (Linan et al., 2008) and other members of the MBGH, 2) directly link strategic business initiatives with employee health needs and 3) concentrate their efforts on increasing employee participation and engagement. Table 4 shows the rate of employee participation in biometric screenings Table 1 describes the companies that completed the self-assessment FIGURE 1. EMPLOYEE AND PARTICIPATION Table 2. RATINGS OF LEADERSHIP SUPPORT X bar 69% Figure 1 shows the self-reported rates of participation and engagement in companies Table 2 shows the self-assessed rate of leadership support for worksite health programming TABLE 5. BARRIERS AND SOLUTIONS Table 3. EMPLOYEE PARTICIPATION FIGURE 2. STAKEHOLDERS CONCERNED WITH WORKSITE HEALTH PROMOTION PROGRAMMING Table 3 shows the rate of employee completion of an HRA and participation in programming n the 24 months prior to the self-assessment. References Edington, D. (2013). Zero Trends. Ann Arbor: MI. Health Management Research Center. Goetzel, R., & Pronk, N. (2010). Worksite Health Promotion. How much do we really know about what works? American Journal of Preventive Medicine, 38, S223-225. Linan et al. (2008). Results of the National Worksite Health Promotion Survey. American Journal of Public Health, 98, 1503-1509. Pronk, N., & Kottke (2009). Physical activity promotion as a strategic corporate priority to improve worker health and business performance . Preventive Medicine, 49, 316-321. Pronk, N. (2009). ACSM’s Worksite Health Handbook, 2nd . Champaign: IL. Human Kinetics. Reavely et al. (2010). A systematic grounded approach to the development of complex interventions: The Australian WorkHealth Program-Arthritis case study. Social Science & Medicine, 70, 342-350. Selby et al. (2010). Barriers to participation in a worksite wellness program. Nutrition Research and Practice, 4, 149-154. Soler et al. (2010). A systematic review of selected interventions for worksite health promotion. American Journal Preventive Medicine, 38, S237-S262. Table 5 shows the prominent barriers to employee participation and solutions recommended in Edington (2013) and Pronk (2009). This figure shows the different internal and external stakeholders involved with program development, delivery and evaluation. Positive numbers are on the left e.g. 14 out of 18 companies reported positive leadership engagement.