Download
1 / 43
490 likes | 1.25k Views
Total Parenteral Nutrition (TPN). By: E. Salehifar (Clinical Pharmacist). Malnutrition. Incidence: 50 % of hospitalized patients Common causes: - Hypermetabolic states: Trauma, Infection, Major surgery, Burn - Poor nutrition

E N D
Total Parenteral Nutrition (TPN) By: E. Salehifar (Clinical Pharmacist)
Malnutrition • Incidence: 50 % of hospitalized patients • Common causes: - Hypermetabolic states: Trauma, Infection, Major surgery, Burn - Poor nutrition • Consequences: Weakness, Decreased wound healing, increased respiratory failure, decreased cardiac contractility, infections (pneumonia, abscesses), Prolonged hospitalization
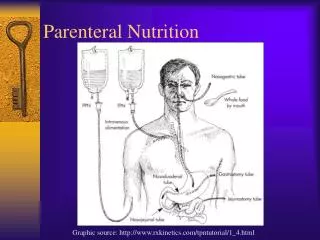
Nutritional Support • Enteral Nutrition ( Physiologic, less expensive) • Parenteral Nutrition - GI should not be used (Obstruction, Pancraitis) - GI can not be used ( Vomiting, Diarrhea, Resection of intestine, IBD)
Parenteral Nutrition • Peripheral Parenteral Nutrition (15 lit D5W/day for a 70 kg !!!) • Central Parenteral Nutrition (TPN) • Needs CV-line to administer hyperosmolar solutions
Estimation of energy expenditure Harris-Benedict equations: • BEE (men) (kcal/day): 66.47+13.75W+5H-6.76A • BEE (women) (kcal/day): 655.1+9.56W+1.85H-4.68A • TEE (kcal/day): BEE × Stress factor × Activity factor • Stress factors: Surgery, Infection: 1.2 Trauma: 1.5 Sepsis: 1.6 Burns: 1.6-2 • Activity factors: sedentary: 1.2 , normal activity: 1.3, active: 1.4 , very active: 1.5
Stress level • Normal/mild stress level: 20-25 kcal/kg/day • Moderate stress level: 25-30 kcal/kg/day • Severe stress level: 30-40 kcal/kg/day • Pregnant women in second or third trimester: Add an additional 300 kcal/day
Fluid: mL/day 30-40 mL/kg
Protein (amino acids) Maintenance: 0.8-1 g/kg/day Normal/mild stress level: 1-1.2 g/kg/day Moderate stress level: 1.2-1.5 g/kg/day Severe stress level: 1.5-2 g/kg/day Burn patients (severe): Increase protein until significant wound healing achieved Solid organ transplant: Perioperative: 1.5-2 g/kg/day
Protein need in Renal failure Acute (severely malnourished or hypercatabolic): 1.5-1.8 g/kg/day Chronic, with dialysis: 1.2-1.3 g/kg/day Chronic, without dialysis: 0.6-0.8 g/kg/day Continuous hemofiltration: ≥ 1 g/kg/day
Protein need in Hepatic failure • Acute management when other treatments have failed: • With encephalopathy: 0.6-1 g/kg/day • Without encephalopathy: 1-1.5 g/kg/day • Chronic encephalopathy • Use branch chain amino acid enriched diets only if unresponsive to pharmacotherapy • Pregnant women in second or third trimester • Add an additional 10-14 g/day
Fat • Initial: 20% to 40 % of total calories (maximum: 60% of total calories or 2.5 g/kg/day) • Note: Monitor triglycerides while receiving intralipids. • Safe for use in pregnancy • I.V. lipids are safe in adults with pancreatitis if triglyceride levels <400 mg/dL
Components of TPN Formulations Macro: Calorie:Dextrose 20%, 50% Intralipid 10%, 20% Protein:Aminofusion 5%, 10% Micro: Electrolytes (Na, K, Mg, Ca, PO4) Trace elements (Zn, Cu, Cr, Mn, Se)
Dextrose • 20%, 50% ( from CV-line) • 3.4 kcal/g • 60-70% of calorie requirements should be provided with dextrose
Dextrose: Contraindications Hypersensitivity to corn or corn products Hypertonic solutions in patients with intracranial or intraspinal hemorrhage
Abrupt withdrawal Infuse 10% dextrose at same rate and monitor blood glucose for hypoglycemia
Intralipid • 10%, 20% ( from peripheral or CV-line) • 1.1 kcal/ml (10%), 2 kcal/ml (20%) • 30-40% of calorie requirements should be provided with Intralipid
1022 Kcal/L 345 mosmol/L 1080 Kcal/L
Intralipid: Contraindication Hypersensitivity to fat emulsion or any component of the formulation; severe egg or legume (soybean) allergies Pathologic hyperlipidemia, lipoid nephrosis, pancreatitis with hyperlipemia (TG>400 mg/dl)
Aminofusion • 5%, 10% ( from CV-line) • 1-1.5 g/kg/day • Should not be used as a calorie source
200 kcal/L 590 mosmol/L 400 Kcal/L 1030 mosmol/L
Amino acids: Contraindications Hypersensitivity to one or more amino acids Severe liver disease or hepatic coma
Case • D.C a 38 y.o man with a 12-year history ofcrohn’s disease is admitted to surgery ward of Imam hospital in Sari for a compliant of increasing abdominal pain, nausea & vomitingfor 7 daysand no stool output for 5 days. Because of N & V, he has been drinking only liquids during the past weeks. His crohn disease had several exacerbations during the past 2 years and 10 cm of his ileum has been resected6 month ago.
case (continue) Drugs: Mesalamine 1000 mg qid + prednisolone 10mg/d. Abdominal x-ray is consisting with bowel obstruction. Exploratory laparotomy was performed and 25 cm of his ileum resected.Bowel sounds are absent. He has a right subclavianCV-line. Considering that his Ht=180cm, Wt=60kg (6 month ago: 70 kg) andAge=38 y.o, what is your recommended TPN formula for him?
BEE= 66.47+13.75×60+5×180-6.76×38=1535 kcal/d • TEE= 1535×1.2×1.2 = 2200 kcal/d • Intralipid 10%= ? 2200 × 30%= 660 kcal 1ml ≡ 1.1 kcal 660 : 1.1 = 600 ml ( 500ml) • Dext 50%= ? 2200 – 550= 1650 kcal 1g dextrose ≡ 3.4 kcal 1650 : 3.4= 485 g Dext 50g ≡ 100 ml 485 g ≡ 970ml (1000ml) • Aminofusion 10 %= ? 1.5 g/kg/d × 60 kg= 90g/day 10g ≡ 100 ml 90g ≡900 ml (1000ml)
Electrolytes (daily requirements for TPN): • Na: 80-100 mEq (50 - 100 ml NaCl 5%) • K: 60-80 mEq (30 ml KCl) • Cl: 50-100 mEq • Mg: 8-16 mEq (5 -10 ml MgSo4 20%) • Ca: 5-10 mEq (10-20 ml Ca Gluconate 10%) • P04: 15-30 mEq • Acetate: 50-100 mEq
Vitamins: A, D, E, Water soluble vitamins • Trace Elements: • Zn, Se, Cu, Cr, Mn • ↓ Zn • Delayed ulcer healing, Dermatitis, Alopcia (5αreductase), Diarrhea • ↓ Se: Low activity of SOD & Deiodinase • Amp B Complex + Amp Vit C MV Therapeutic ( Zn, Cu, Mn)
Special Considerations • Max infusion rate of dextrose: 0.5g/kg/h (to avoid hyperglycemia, glycosuria, fatty liver, hyperosmolar coma) • K should be added to dextrose solutions • Slow starting & slow tapering of Dext 50% • If BS>200, Insulin should be added • some brands of lipids can be mixed with Dext+Aminifusion in the same IV container
Special Considerations • Intralipid contraindications: • Severe egg allergy • Hyperlipidemia • Special aminoacid products: • Hepatamine: for Hepatic Failure • ↑ branched chain aa ( leu, isoleu, val) • Nephramine: for Renal Failure • Primarily essential aa with lower concentrations
Monitoring: • Baseline:Wt, Na, K, BUN, Cr, Glu, Ca, P, Mg, CBC, PT, INR, TG, LFT, Alb, Pre-Alb • Daily:Wt, V/S, I-O, Na, K, BUN, Cr, Glu, Sign/Symptoms of infection • 2-3 times a week:CBC, Ca, P, Mg • Weekly:Alb, Pre-Alb, LFT, INR, Nitrogen Balance
Adding other drugs to TPN • INS • Heparin • H2-blocker • Alb • Aminophylline • Vit K & Bicarbonate should not be added
Complications • Endocrine & metabolic • Fluid overload, hypercapnia, hyperglycemia, hyper-/hypokalemia, hyper-/hypophosphatemia, refeeding syndrome • Hepatic • Cholestasis, cirrhosis (<1%), gallstones, liver function tests increased, pancreatitis, steatosis, triglycerides increased • Renal • Azotemia, BUN increased • Infectious • Bacteremia, catheter-induced infection, exit-site infections • Other: Pneumothorax, Thrombophlebitis
Refeeding syndrome • In patients with long-standing or severe malnutrition • Is a medical emergency, consist of: • Electrolyte disturbances (eg, potassium, phosphorus) • Respiratory distress • Cardiac arrhythmias, resulting in cardiopulmonary arrest • Do not overfeed patients; caloric replacement should match as closely as possible to intake
Conclusion • Malnutrition is a common problem & Nutritional support is indicated in many hospitalized patients • Enteral nutrition is better, but some patients with GI problems need TPN • Dextrose & Intralipid should be used as calorie sources and Aminofusion as aminoacid source • Special monitoring should be considered for patients especially I-O, Na, K and Glu